
Whenever you need to fill out da treatment sheet sample, you won't have to download and install any sort of software - simply use our online tool. Our development team is constantly endeavoring to develop the tool and enable it to be even easier for users with its handy features. Enjoy an ever-evolving experience today! Starting is easy! All you should do is take the following easy steps below:
Step 1: Press the orange "Get Form" button above. It will open up our tool so you could start filling in your form.
Step 2: With the help of our handy PDF editor, you may do more than just fill out blank form fields. Try each of the features and make your docs look high-quality with custom textual content added, or modify the original input to perfection - all comes with an ability to add any pictures and sign the document off.
This document requires specific info to be filled in, so you need to take some time to fill in what's expected:
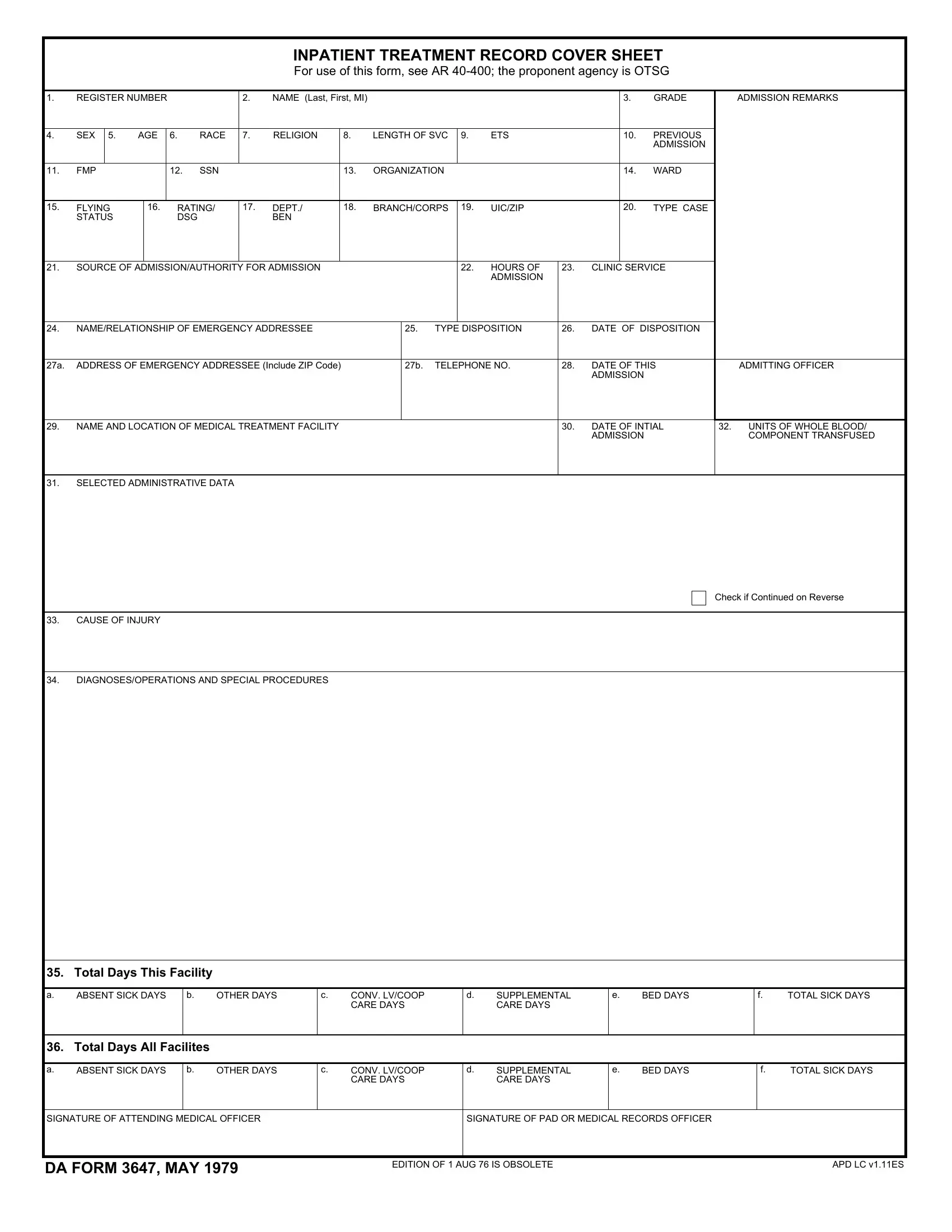
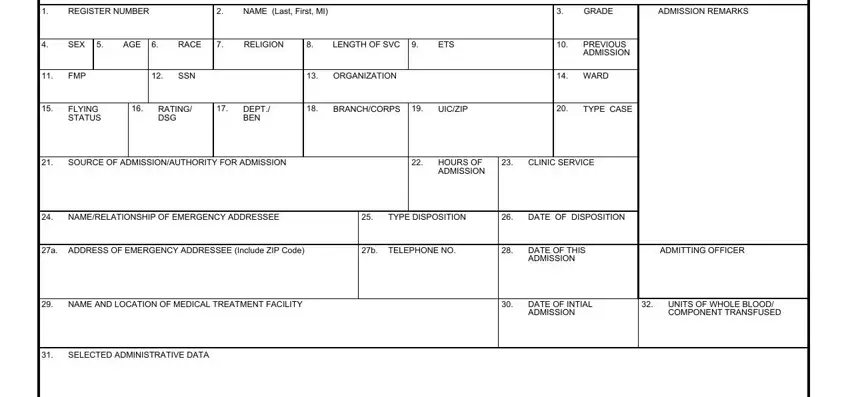
1. The da treatment sheet sample requires particular details to be inserted. Make sure the subsequent fields are completed:
2. Once your current task is complete, take the next step – fill out all of these fields - CAUSE OF INJURY, DIAGNOSESOPERATIONS AND SPECIAL, Check if Continued on Reverse, Total Days This Facility, ABSENT SICK DAYS, OTHER DAYS, CONV LVCOOP CARE DAYS, SUPPLEMENTAL CARE DAYS, BED DAYS, and TOTAL SICK DAYS with their corresponding information. Make sure to double check that everything has been entered correctly before continuing!
3. The next step is normally easy - complete all the empty fields in ABSENT SICK DAYS, OTHER DAYS, CONV LVCOOP CARE DAYS, SUPPLEMENTAL CARE DAYS, BED DAYS, TOTAL SICK DAYS, SIGNATURE OF ATTENDING MEDICAL, SIGNATURE OF PAD OR MEDICAL, DA FORM MAY, EDITION OF AUG IS OBSOLETE, and APD LC vES to conclude this segment.

Regarding BED DAYS and SIGNATURE OF PAD OR MEDICAL, ensure that you get them right in this current part. Both of these are thought to be the most significant fields in this page.
Step 3: Check that your information is correct and click on "Done" to complete the task. Join us today and instantly obtain da treatment sheet sample, available for download. Each and every edit you make is handily saved , which means you can modify the form further if required. We don't share or sell the details that you enter whenever working with documents at our site.