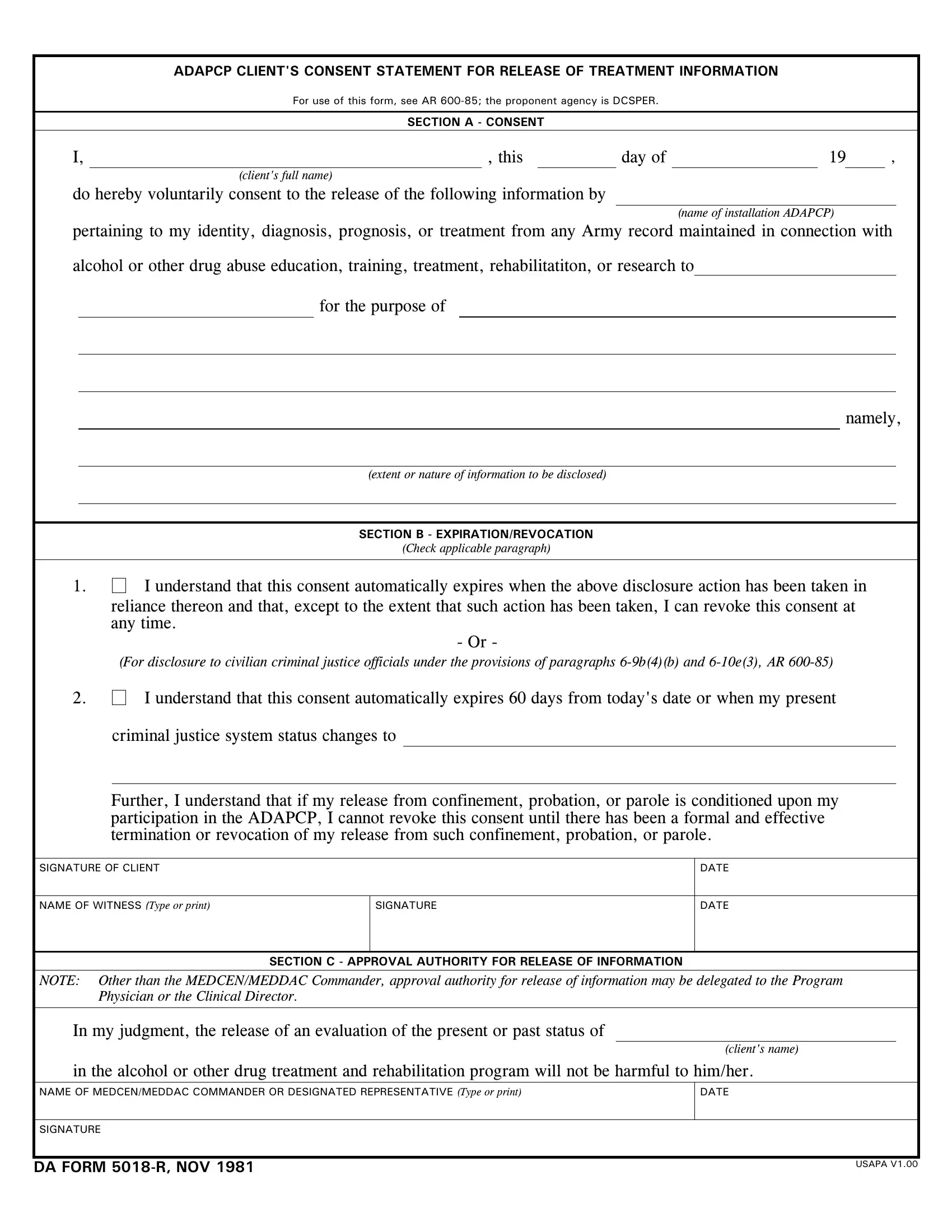
The DA 5018 R form, titled "ADAPCP Client's Consent Statement for Release of Treatment Information," serves a crucial function within the framework of the Army's Alcohol and Drug Abuse Prevention and Control Program (ADAPCP). It is designed to safeguard the privacy of individuals receiving treatment for alcohol or other drug abuse by ensuring that any release of their treatment information is consensual. The form encapsulates various sections, including the client's consent, where the individual voluntarily agrees to the disclosure of specific information related to their diagnosis, prognosis, or treatment. Additionally, it sheds light on the conditions under which the consent expires or can be revoked, emphasizing the autonomy of the client in the management of their personal information. Furthermore, with section B outlining stipulations for expiration and revocation, especially in the context of interactions with civilian criminal justice officials, it underscores the protective measures in place for clients navigating both health and legal systems. Approval authority, as described in section C, ensures that any information release is deemed non-harmful to the client, thereby embedding an extra layer of consideration and care into the process. Through this form, the army not only demonstrates its commitment to the privacy and well-being of individuals undergoing treatment but also aligns with broader principles of confidentiality and ethical responsibility in healthcare.
| Question | Answer |
|---|---|
| Form Name | DA Form 5018-R |
| Form Length | 1 pages |
| Fillable? | Yes |
| Fillable fields | 1 |
| Avg. time to fill out | 27 sec |
| Other names | da 5018 r fillable, da form 5018 r pdf, form adapcp form, da form 5018 r fillable |
ADAPCP CLIENT'S CONSENT STATEMENT FOR RELEASE OF TREATMENT INFORMATION
For use of this form, see AR
SECTION A - CONSENT
I, |
, this |
day of |
19 |
, |
(client's full name)
do hereby voluntarily consent to the release of the following information by
(name of installation ADAPCP)
pertaining to my identity, diagnosis, prognosis, or treatment from any Army record maintained in connection with
alcohol or other drug abuse education, training, treatment, rehabilitatiton, or research to
for the purpose of
namely,
(extent or nature of information to be disclosed)
SECTION B - EXPIRATION/REVOCATION
(Check applicable paragraph)
1. I understand that this consent automatically expires when the above disclosure action has been taken in
reliance thereon and that, except to the extent that such action has been taken, I can revoke this consent at any time.
- Or -
(For disclosure to civilian criminal justice officials under the provisions of paragraphs
2.
I understand that this consent automatically expires 60 days from today's date or when my present
criminal justice system status changes to
Further, I understand that if my release from confinement, probation, or parole is conditioned upon my participation in the ADAPCP, I cannot revoke this consent until there has been a formal and effective termination or revocation of my release from such confinement, probation, or parole.
SIGNATURE OF CLIENT
DATE
NAME OF WITNESS (Type or print)
SIGNATURE
DATE
SECTION C - APPROVAL AUTHORITY FOR RELEASE OF INFORMATION
NOTE: Other than the MEDCEN/MEDDAC Commander, approval authority for release of information may be delegated to the Program Physician or the Clinical Director.
In my judgment, the release of an evaluation of the present or past status of
(client's name)
in the alcohol or other drug treatment and rehabilitation program will not be harmful to him/her.
NAME OF MEDCEN/MEDDAC COMMANDER OR DESIGNATED REPRESENTATIVE (Type or print)
DATE
SIGNATURE
DA FORM
USAPA V1.00