
Using the online PDF tool by FormsPal, it is possible to fill in or alter cdac record right here. Our editor is consistently evolving to deliver the very best user experience possible, and that's thanks to our resolve for continuous improvement and listening closely to comments from users. In case you are seeking to get started, here's what you will need to do:
Step 1: Click the "Get Form" button above. It will open our pdf tool so you could start filling in your form.
Step 2: Using this online PDF editor, you are able to do more than merely fill out blanks. Express yourself and make your forms appear sublime with customized text added in, or modify the original input to perfection - all that supported by the capability to add your personal images and sign the PDF off.
Filling out this form needs attention to detail. Ensure that each blank field is filled out accurately.
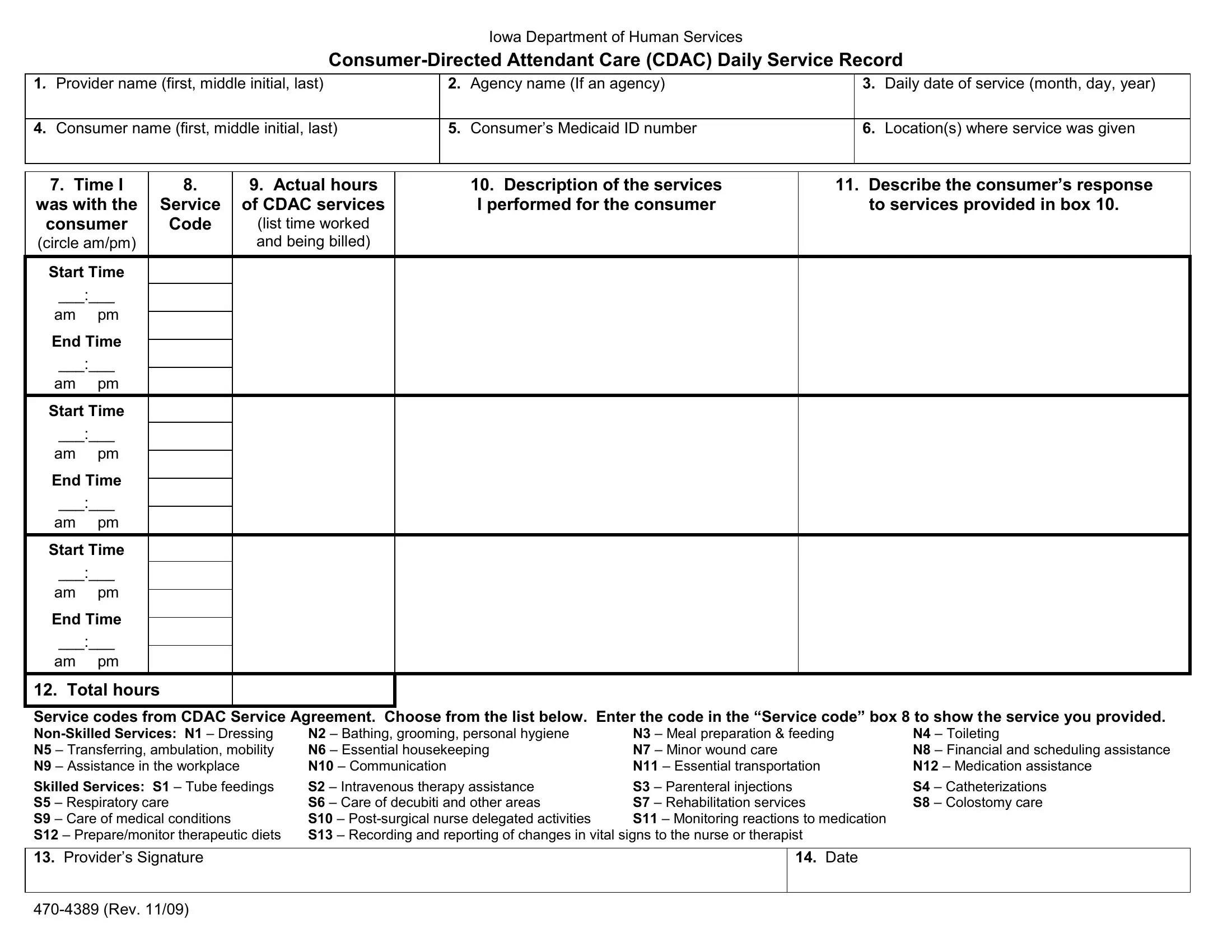
1. You will need to complete the cdac record properly, thus be attentive while working with the parts that contain these blanks:
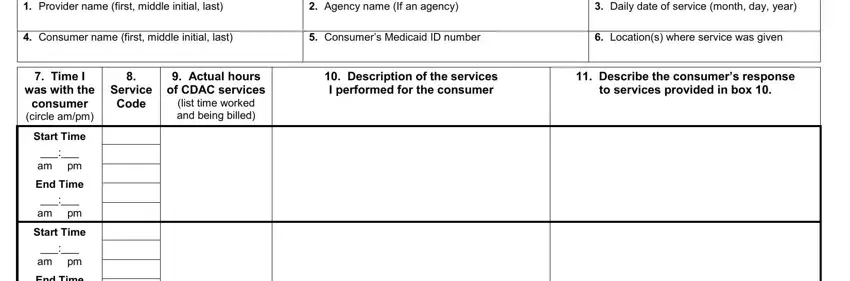
2. The next step is to submit the following fields: am pm End Time am pm Start Time, am pm, End Time, am pm, Total hours Service codes from, N Bathing grooming personal, N Meal preparation feeding N, N Toileting N Financial and, Date, and Rev.
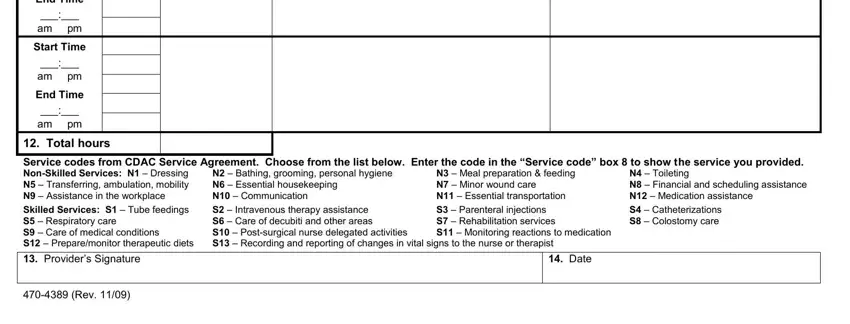
Be very mindful while filling out am pm End Time am pm Start Time and am pm, because this is where many people make a few mistakes.
Step 3: Prior to finalizing your form, make certain that all blank fields were filled out the right way. The moment you believe it's all fine, click “Done." Sign up with us today and instantly use cdac record, all set for download. All adjustments you make are saved , making it possible to customize the document at a later stage as required. FormsPal ensures your information confidentiality by having a protected method that in no way saves or shares any kind of private information provided. Be assured knowing your documents are kept confidential any time you use our tools!