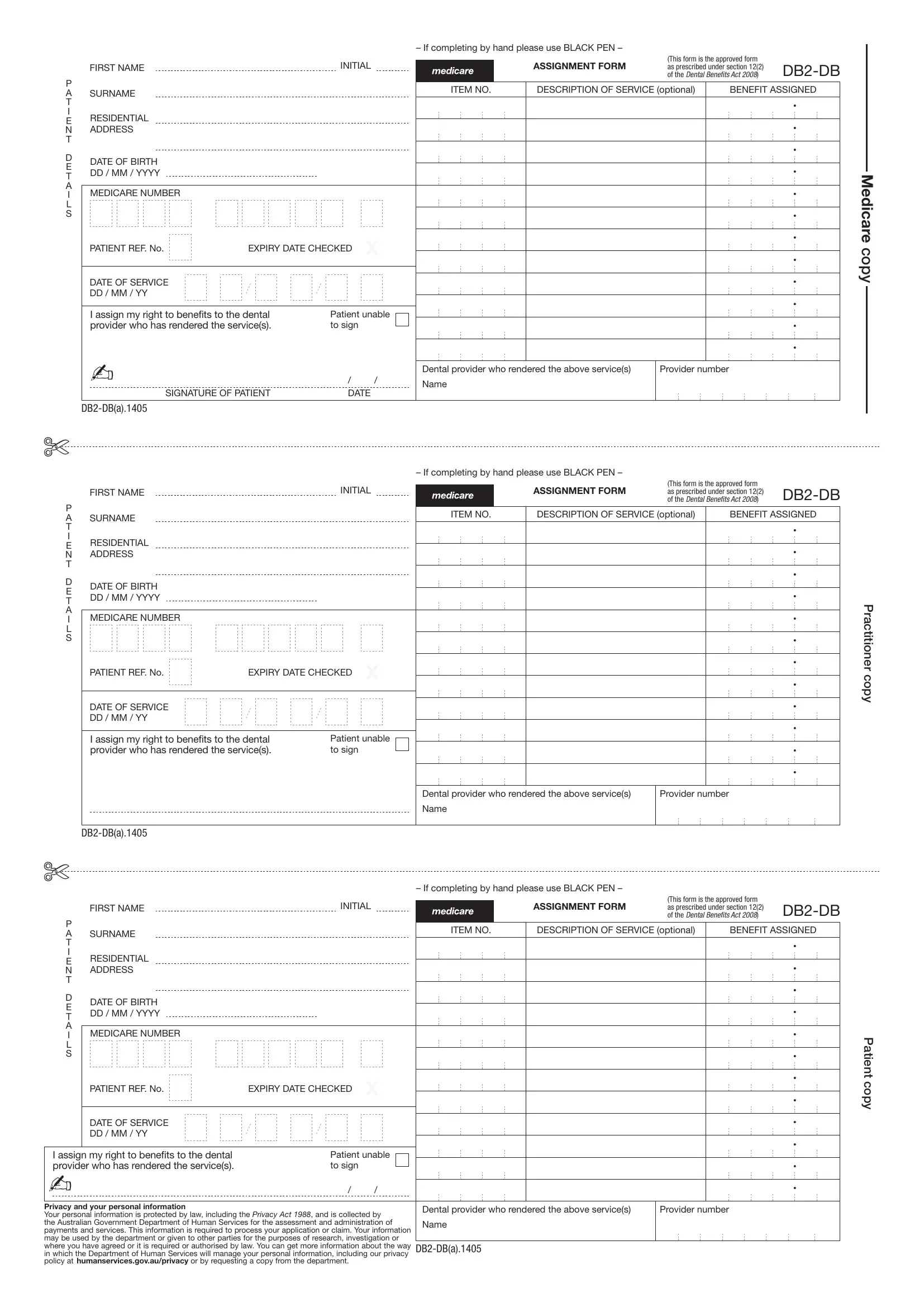
The Db2 Assignment form plays a critical role in the administration of dental benefits under the DENTAL BENEFITS ACT 2008, serving as a primary document for the assignment of benefits between patients and dental service providers. Instituted by the Australian Government, this form requires completion in black ink and includes several key sections: personal information such as the patient's name, residential address, date of birth, and Medicare number, details of the dental service provided including item numbers and descriptions, and an assignment section where patients can assign their right to benefits directly to the dental provider. This last part is crucial as it facilitates the direct payment of benefits to the providers of dental services, streamlining the process for all parties involved. Furthermore, the form contains important prompts regarding the protection of personal information, governed by the Privacy Act 1988, ensuring that patients' data is handled with the utmost confidentiality and security by the Department of Human Services. Through clear instructions and fields, the Db2 Assignment form embodies an essential tool in the efficient management and assignment of dental benefits, making it easier for both the service providers and patients to navigate the intricacies of healthcare services administration.
| Question | Answer |
|---|---|
| Form Name | Db2 Assignment Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | form db2 db, db2 ot forms from medicare, online 888 form fill, medicare australia forms |
– If completing by hand please use BLACK PEN –
|
|
|
INITIAL |
|
|
ASSIGNMENT FORM |
(This form is the approved form |
|
||
|
FIRST NAME |
|
|
|
as prescribed under section 12(2) |
|||||
|
|
|
|
|
|
|
|
of the DENTAL BENEfiTS ACT 2008) |
||
P |
|
|
|
|
|
ITEM NO. |
DESCRIPTION OF SERVICE (optional) |
BENEFIT ASSIGNED |
||
A |
SURNAME |
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
||
T |
|
|
|
|
|
|
|
|
|
• |
I |
|
|
|
|
|
|
|
|
|
|
RESIDENTIAL |
|
|
|
|
|
|
|
|
|
|
E |
|
|
|
|
|
|
|
|
|
|
ADDRESS |
|
|
|
|
|
|
|
|
• |
|
N |
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
||
T |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
• |
D |
DATE OF BIRTH |
|
|
|
|
|
|
|
|
|
E |
|
|
|
|
|
|
|
|
|
|
DD / MM / YYYY |
|
|
|
|
|
|
|
|
• |
|
T |
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
A |
MEDICARE NUMBER |
|
|
|
|
|
|
|
|
• |
I |
|
|
|
|
|
|
|
|
||
L |
|
|
|
|
|
|
|
|
|
|
S |
|
|
|
|
|
|
|
|
|
• |
|
|
|
|
X |
|
|
|
|
• |
|
|
PATIENT REF. No. |
EXPIRY DATE CHECKED |
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
• |
|
DATE OF SERVICE |
|
|
|
|
|
|
|
|
• |
|
DD / MM / YY |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
• |
|
I assign my right to benefits to the dental |
Patient unable |
|
|
|
|
|
|||
|
provider who has rendered the service(s). |
to sign |
|
|
|
|
|
|
• |
|
|
|
|
|
|
|
|
|
|
|
• |
|
- |
|
|
|
|
Dental provider who rendered the above service(s) |
Provider number |
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
/ |
|
/ |
Name |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
SIGNATURE OF PATIENT |
DATE |
|
|
|
|
|
|
||
Medicare copy
$
– If completing by hand please use BLACK PEN –
(This form is the approved form
FIRST NAMEINITIALASSIGNMENT FORMas prescribed under section 12(2)
P |
|
ITEM NO. |
DESCRIPTION OF SERVICE (optional) |
BENEFIT ASSIGNED |
A |
SURNAME |
|||
T |
|
|
|
• |
I |
|
|
|
|
ERESIDENTIAL
N |
ADDRESS |
|
|
|
• |
|
|
|
|
||
T |
|
|
|
|
|
|
|
|
|
|
• |
D |
DATE OF BIRTH |
|
|
|
|
E |
|
|
|
|
|
DD / MM / YYYY |
|
|
|
• |
|
T |
|
|
|
||
|
|
|
|
|
|
A |
MEDICARE NUMBER |
|
|
|
• |
I |
|
|
|
||
L |
|
|
|
|
|
S |
|
|
|
|
• |
|
|
|
|
X |
• |
|
PATIENT REF. No. |
EXPIRY DATE CHECKED |
|
||
|
|
|
|||
|
|
|
|
|
• |
|
DATE OF SERVICE |
|
|
|
• |
|
DD / MM / YY |
|
|
|
|
|
|
|
|
|
• |
|
I assign my right to benefits to the dental |
Patient unable |
|
||
|
provider who has rendered the service(s). |
to sign |
|
• |
|
|
|
|
|
|
• |
|
|
|
|
Dental provider who rendered the above service(s) |
Provider number |
|
|
|
|
Name |
|
Practitioner copy
$
– If completing by hand please use BLACK PEN –
(This form is the approved form
FIRST NAMEINITIALASSIGNMENT FORMas prescribed under section 12(2)
P |
|
ITEM NO. |
DESCRIPTION OF SERVICE (optional) |
BENEFIT ASSIGNED |
A |
SURNAME |
|||
T |
|
|
|
• |
I |
|
|
|
|
ERESIDENTIAL
N |
ADDRESS |
|
|
• |
|
|
|
||
T |
|
|
|
|
|
|
|
|
• |
D |
DATE OF BIRTH |
|
|
|
E |
|
|
|
|
DD / MM / YYYY |
|
|
• |
|
T |
|
|
||
|
|
|
|
|
A |
MEDICARE NUMBER |
|
|
• |
I |
|
|
||
L |
|
|
|
|
S |
|
|
|
• |
|
|
|
X |
• |
|
PATIENT REF. No. |
EXPIRY DATE CHECKED |
|
|
|
|
|
||
|
|
|
|
• |
|
DATE OF SERVICE |
|
|
• |
|
DD / MM / YY |
|
|
|
|
|
|
|
• |
I assign my right to benefits to the dental |
Patient unable |
|
||
provider who has rendered the service(s). |
to sign |
|
• |
|
- |
|
|
|
|
|
/ |
/ |
|
• |
||
|
|
|
|
|
|
Privacy and your personal information |
|
|
Dental provider who rendered the above service(s) |
Provider number |
|
Your personal information is protected by law, including the Privacy Act 1988, and is collected by |
|||||
|
|
||||
the Australian Government Department of Human Services for the assessment and administration of |
Name |
|
|||
payments and services. This information is required to process your application or claim. Your information |
|
|
|||
may be used by the department or given to other parties for the purposes of research, investigation or |
|
|
|||
where you have agreed or it is required or authorised by law. You can get more information about the way |
|
||||
in which the Department of Human Services will manage your personal information, including our privacy |
|
|
|||
policy at humanservices.gov.au/privacy or by requesting a copy from the department.
Patient copy