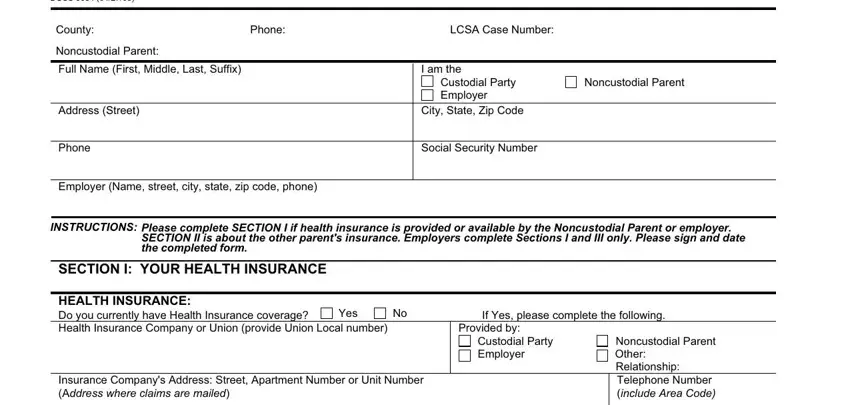
 Yes If Yes, please complete the following information.
Yes If Yes, please complete the following information.
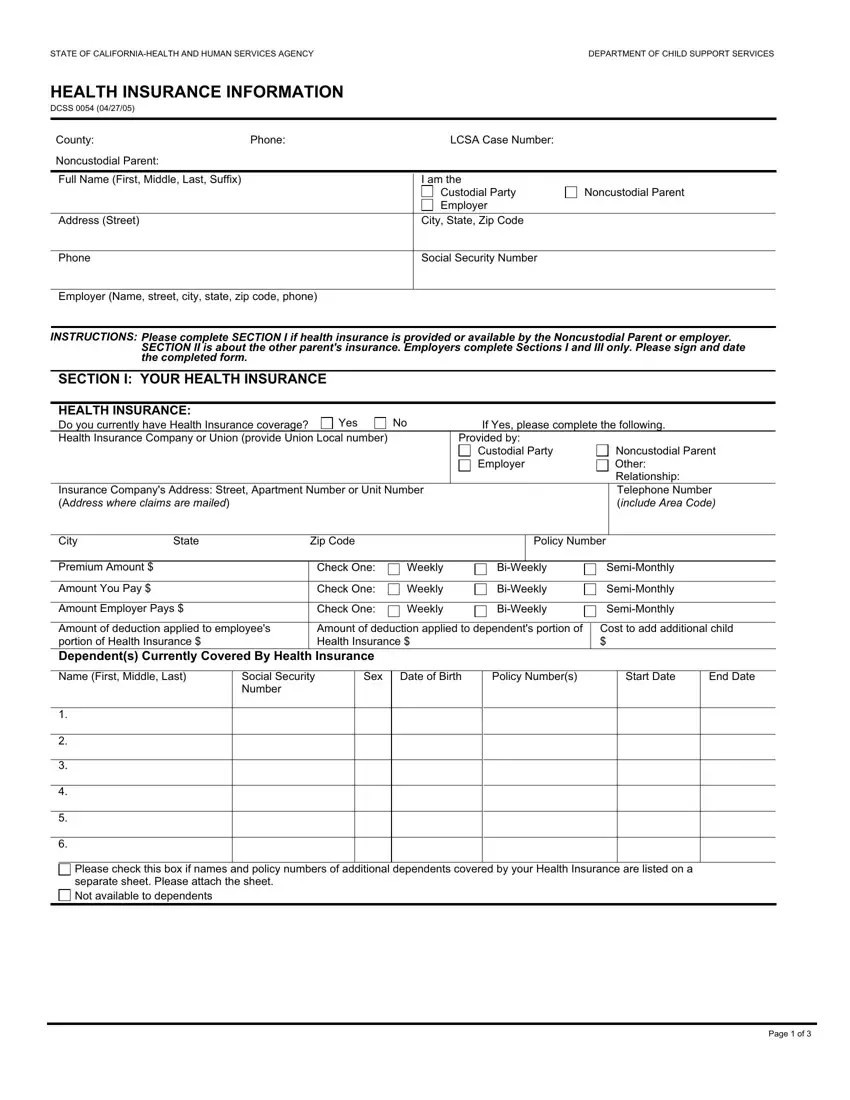
 At this time there is no health insurance coverage available. I understand that if it becomes available, I will have to add my child(ren) onto the plan and then notify the local child support agency of the coverage. Coverage is unavailable because:
At this time there is no health insurance coverage available. I understand that if it becomes available, I will have to add my child(ren) onto the plan and then notify the local child support agency of the coverage. Coverage is unavailable because:It really is very easy to fill in the dcss health insurance information. Our software was intended to be assist you to prepare any PDF easily. These are the actions to go through:
Step 1: Find the button "Get Form Here" on this website and hit it.
Step 2: At the moment you're on the file editing page. You may modify and add text to the document, highlight specified content, cross or check particular words, include images, insert a signature on it, erase unneeded areas, or remove them entirely.
Enter the appropriate material in every section to prepare the PDF dcss health insurance information
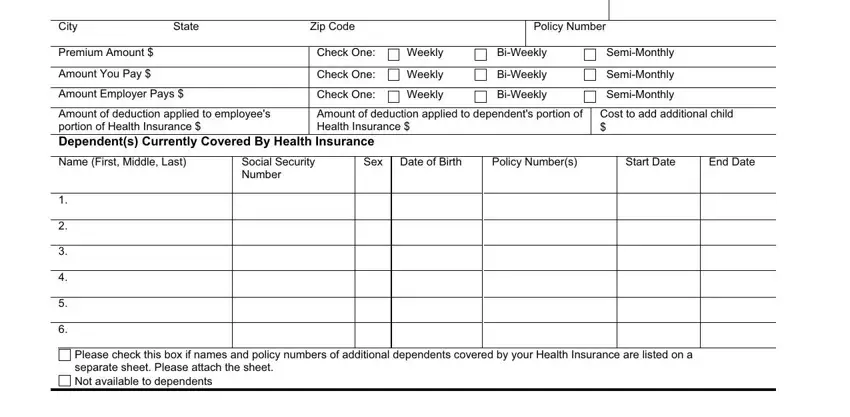
Indicate the data in City, State, Zip Code, Policy Number, Premium Amount, Amount You Pay, Amount Employer Pays, Check One, Weekly, Check One, Check One, Weekly, Weekly, BiWeekly, and BiWeekly.
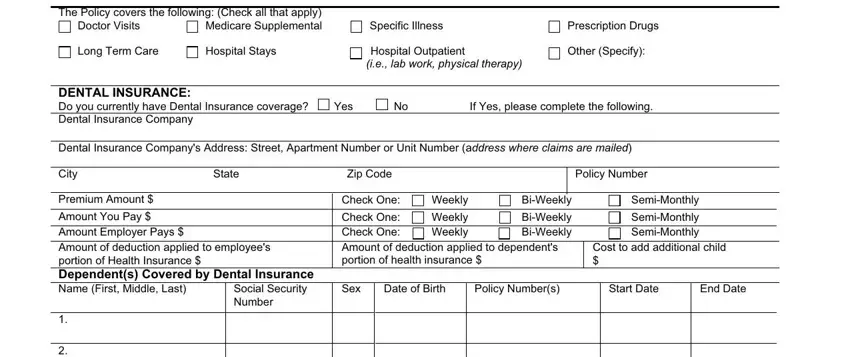
You'll be expected to provide the details to help the application complete the box The Policy covers the following, Doctor Visits, Long Term Care, Hospital Stays, DENTAL INSURANCE Do you currently, Specific Illness, Prescription Drugs, Hospital Outpatient ie lab work, Other Specify, Yes, If Yes please complete the, Dental Insurance Companys Address, City, State, and Zip Code.
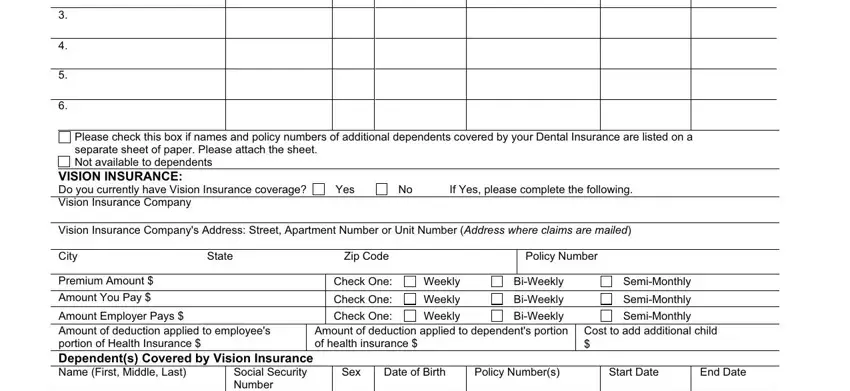
Indicate the rights and obligations of the parties within the paragraph Please check this box if names and, VISION INSURANCE Do you currently, Yes, If Yes please complete the, Vision Insurance Companys Address, City, State, Zip Code, Policy Number, Premium Amount Amount You Pay, Check One, Check One, Weekly, Weekly, and BiWeekly.
Look at the fields Amount Employer Pays Amount of, Please check this box if names and, HEALTH INSURANCE INFORMATION DCSS, and Page of and thereafter fill them in.
Step 3: Choose the Done button to save the form. So now it is available for export to your device.
Step 4: Just be sure to generate as many duplicates of your document as you can to avoid future problems.
