
Whenever you would like to fill out dd form 137 7, it's not necessary to download any software - simply use our online tool. FormsPal team is aimed at providing you with the absolute best experience with our tool by regularly presenting new functions and improvements. With all of these updates, using our tool becomes easier than ever! If you are looking to get started, here is what it requires:
Step 1: Access the PDF file in our editor by pressing the "Get Form Button" in the top section of this webpage.
Step 2: This editor grants the opportunity to modify your PDF form in a variety of ways. Modify it with your own text, adjust what's originally in the file, and place in a signature - all at your disposal!
This PDF doc needs specific information; in order to ensure consistency, please heed the next recommendations:
1. When filling out the dd form 137 7, make sure to include all of the important blanks within the associated form section. It will help expedite the process, enabling your information to be handled without delay and appropriately.
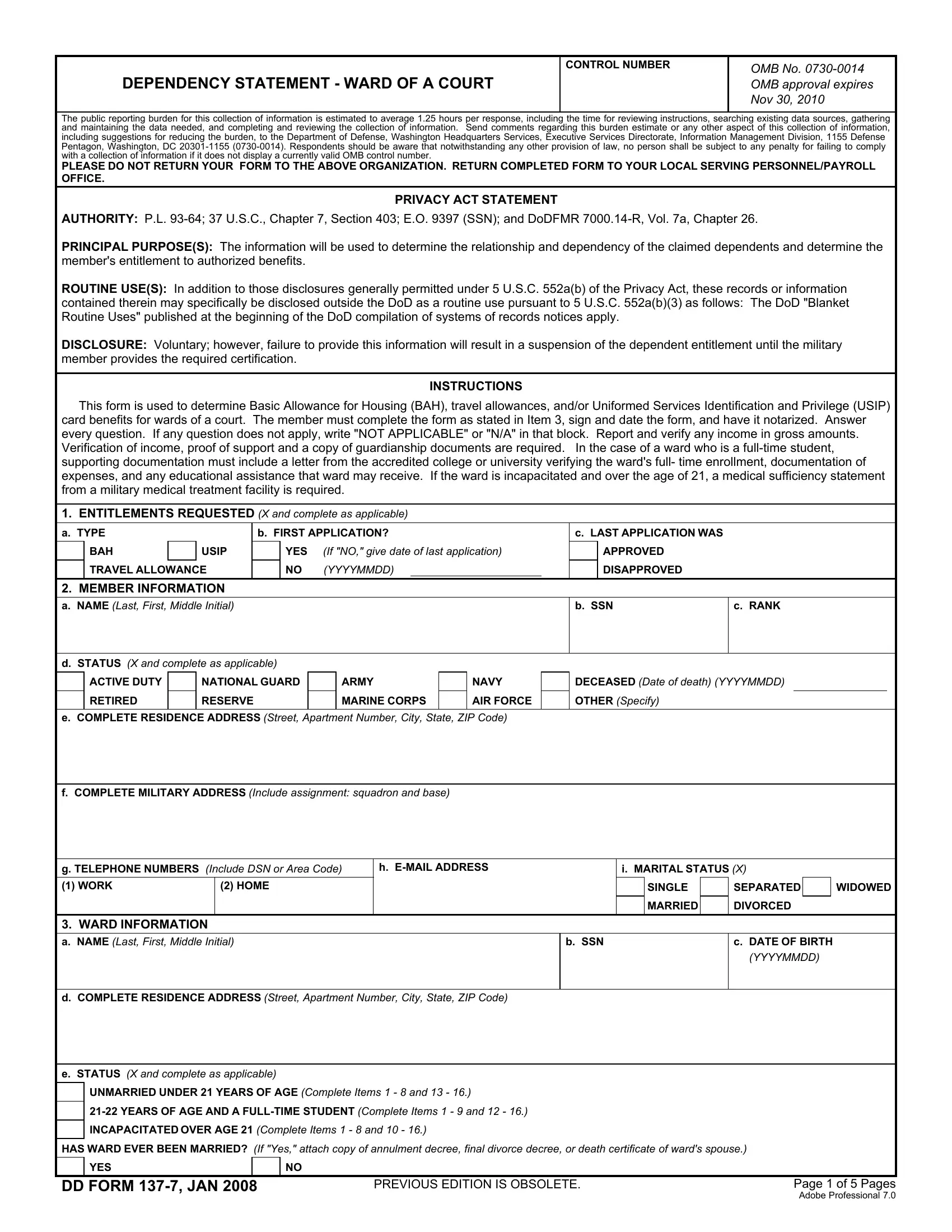
2. Right after completing the last step, head on to the next stage and complete the essential particulars in all these blanks - a NAME Last First Middle Initial, b SSN, c RANK, d STATUS X and complete as, ACTIVE DUTY, NATIONAL GUARD, ARMY, NAVY, DECEASED Date of death YYYYMMDD, RETIRED, RESERVE, MARINE CORPS, AIR FORCE, OTHER Specify, and e COMPLETE RESIDENCE ADDRESS.
3. In this specific stage, review e STATUS X and complete as, UNMARRIED UNDER YEARS OF AGE, YEARS OF AGE AND A FULLTIME, INCAPACITATED OVER AGE Complete, HAS WARD EVER BEEN MARRIED If Yes, YES, DD FORM JAN PREVIOUS EDITION IS, and Page of Pages Adobe Professional. Every one of these will have to be completed with highest precision.

You can certainly get it wrong while filling in your Page of Pages Adobe Professional, hence be sure to reread it before you decide to finalize the form.
4. This specific section arrives with the following fields to consider: WARDS RESIDENCE, a TYPE OF RESIDENCE X and complete, HOME OR APARTMENT OF MEMBER, HOME OR APARTMENT OF WARD, HOME OR APARTMENT OF FRIEND OR, HOME OR APARTMENT OF FORMER SPOUSE, STUDENT DORMITORY OR OTHER, HOSPITAL OR INSTITUTION, b OWNER OF RESIDENCE, OTHER Explain, NAME Last First Middle Initial, ADDRESS Street Apartment Number, c IS RESIDENCE SUBSIDIZED HOUSING, d DATE WARD BEGAN LIVING AT CURRENT, and e DATE WARD BEGAN LIVING WITH.
5. This pdf has to be finalized with this particular area. Further one can find an extensive set of blank fields that need accurate information in order for your form submission to be accomplished: d TYPE OF RESIDENCE X and complete, WARDS OWN HOME OR APARTMENT, MEMBERS HOME OR APARTMENT, HOME OR APARTMENT OF MEMBERS, STUDENT DORMITORY OR OTHER, HOME OR APARTMENT OF FRIEND OR, HOME OR APARTMENT OF MEMBERS WIDOW, OTHER Explain, PERSONS LIVING IN HOUSEHOLD WITH, a NAME Last First Middle Initial, b AGE, c MARRIED X, d EMPLOYED, YES, and HOURS PER WEEK.
Step 3: Once you've looked once again at the details entered, click on "Done" to finalize your document creation. Acquire your dd form 137 7 the instant you sign up at FormsPal for a free trial. Quickly get access to the pdf document in your FormsPal account, together with any edits and changes being automatically saved! FormsPal ensures your data confidentiality by using a protected method that never saves or distributes any type of personal data used in the file. You can relax knowing your docs are kept confidential any time you use our tools!