|
|
|
|
|
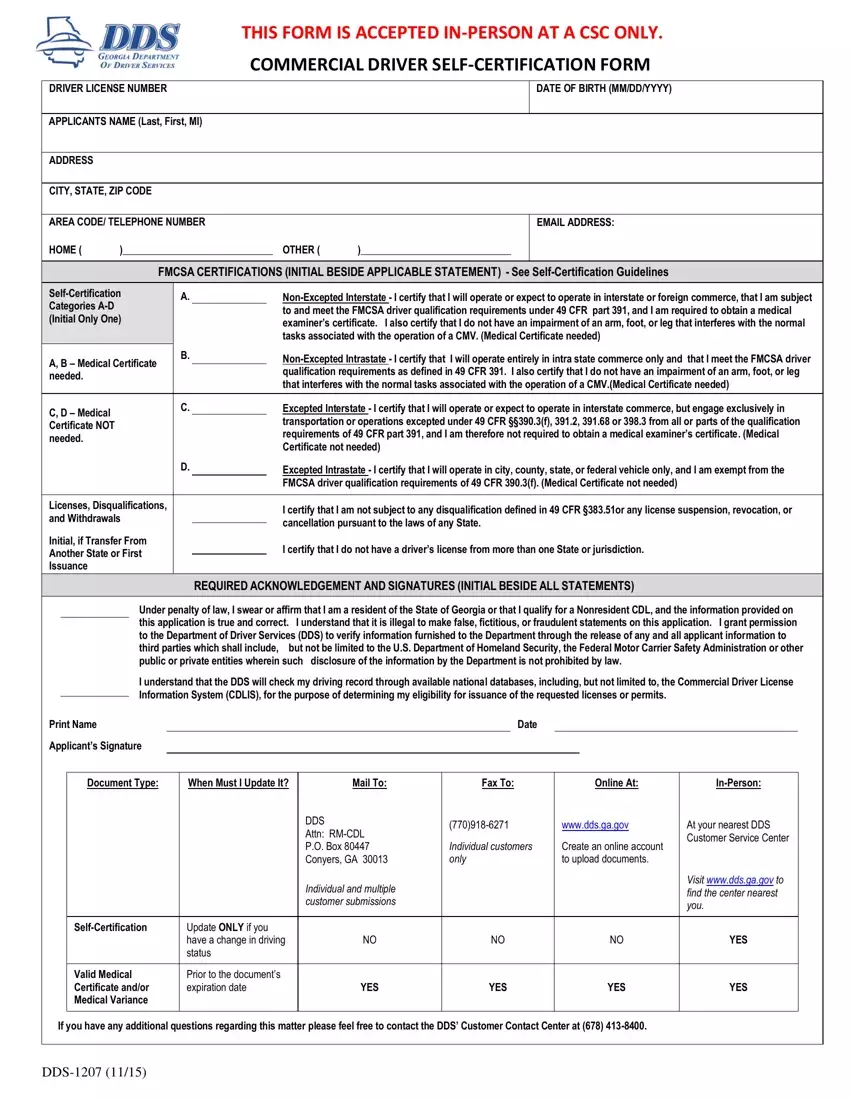
THIS FORM IS ACCEPTED IN-PERSON AT A CSC ONLY. |
|
|
|
|
|
COMMERCIAL DRIVER SELF-CERTIFICATION FORM |
|
|
|
|
|
|
|
|
DRIVER LICENSE NUMBER |
|
|
|
|
|
DATE OF BIRTH (MM/DD/YYYY) |
|
|
|
|
|
|
|
|
APPLICANTS NAME (Last, First, MI) |
|
|
|
|
|
|
|
|
|
|
|
|
|
ADDRESS |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CITY, STATE, ZIP CODE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
AREA CODE/ TELEPHONE NUMBER |
|
|
EMAIL ADDRESS: |
HOME ( |
)______________________________ |
OTHER ( |
)______________________________ |
|
|
|
|
|
|
|
|
|
|
|
|
FMCSA CERTIFICATIONS (INITIAL BESIDE APPLICABLE STATEMENT) - See Self-Certification Guidelines |
Self-Certification |
|
A. |
Non-Excepted Interstate - I certify that I will operate or expect to operate in interstate or foreign commerce, that I am subject |
Categories A-D |
|
|
|
|
|
|
|
to and meet the FMCSA driver qualification requirements under 49 CFR part 391, and I am required to obtain a medical |
(Initial Only One) |
|
|
|
|
|
|
|
|
examiner’s certificate. I also certify that I do not have an impairment of an arm, foot, or leg that interferes with the normal |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
tasks associated with the operation of a CMV. (Medical Certificate needed) |
A, B – Medical Certificate |
B. |
Non-Excepted Intrastate - I certify that I will operate entirely in intra state commerce only and that I meet the FMCSA driver |
|
|
|
|
|
|
qualification requirements as defined in 49 CFR 391. I also certify that I do not have an impairment of an arm, foot, or leg |
needed. |
|
|
|
|
|
|
|
|
|
|
that interferes with the normal tasks associated with the operation of a CMV.(Medical Certificate needed) |
|
|
|
|
|
|
|
|
|
|
|
|
|
C, D – Medical |
|
|
C. |
Excepted Interstate - I certify that I will operate or expect to operate in interstate commerce, but engage exclusively in |
|
|
|
|
|
transportation or operations excepted under 49 CFR §§390.3(f), 391.2, 391.68 or 398.3 from all or parts of the qualification |
Certificate NOT |
|
|
|
|
|
|
|
|
|
|
requirements of 49 CFR part 391, and I am therefore not required to obtain a medical examiner’s certificate. (Medical |
needed. |
|
|
|
|
|
|
|
|
|
|
Certificate not needed) |
|
|
|
|
|
|
|
|
|
|
|
D. |
Excepted Intrastate - I certify that I will operate in city, county, state, or federal vehicle only, and I am exempt from the |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
FMCSA driver qualification requirements of 49 CFR 390.3(f). (Medical Certificate not needed) |
|
|
|
|
|
|
|
|
Licenses, Disqualifications, |
|
|
|
I certify that I am not subject to any disqualification defined in 49 CFR §383.51or any license suspension, revocation, or |
and Withdrawals |
|
|
|
|
|
|
|
|
cancellation pursuant to the laws of any State. |
Initial, if Transfer From |
|
|
|
|
|
|
I certify that I do not have a driver’s license from more than one State or jurisdiction. |
Another State or First |
|
|
|
|
|
|
|
|
|
Issuance |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
REQUIRED ACKNOWLEDGEMENT AND SIGNATURES (INITIAL BESIDE ALL STATEMENTS) |
|
|
|
Under penalty of law, I swear or affirm that I am a resident of the State of Georgia or that I qualify for a Nonresident CDL, and the information provided on |
|
|
|
this application is true and correct. I understand that it is illegal to make false, fictitious, or fraudulent statements on this application. I grant permission |
|
|
|
to the Department of Driver Services (DDS) to verify information furnished to the Department through the release of any and all applicant information to |
|
|
|
third parties which shall include, |
but not be limited to the U.S. Department of Homeland Security, the Federal Motor Carrier Safety Administration or other |
|
|
|
public or private entities wherein such disclosure of the information by the Department is not prohibited by law. |
|
|
|
I understand that the DDS will check my driving record through available national databases, including, but not limited to, the Commercial Driver License |
|
|
|
Information System (CDLIS), for the purpose of determining my eligibility for issuance of the requested licenses or permits. |
|
|
|
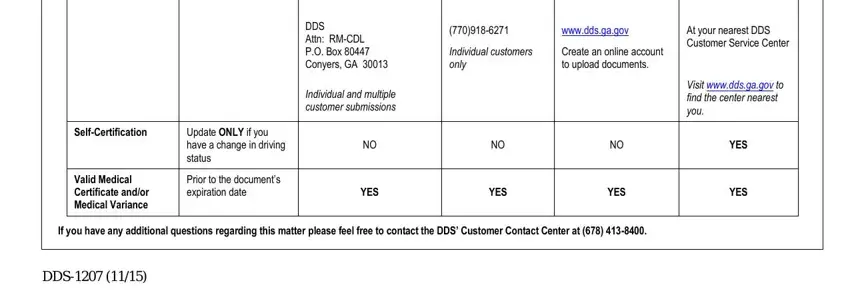
If you have any additional questions regarding this matter please feel free to contact the DDS’ Customer Contact Center at (678) 413-8400.