Delaware Uc 400 is a form that companies in Delaware use to inform the state of their company's organizational structure. This document includes information on the company's officers, directors, and shareholders. Filing this form with the state of Delaware is required for all companies organized under its laws. The form must be filed within 90 days of the company's incorporation or organization. missing this deadline can result in fines and other penalties. For more information on Delaware Form Uc 400, please visit our website or contact us today. We would be happy to help you get started!
| Question | Answer |
|---|---|
| Form Name | Delaware Form Uc 400 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | Delaware, UC-400, dept of labor delaware, delaware rehire credit application form |
Delaware Department of Labor |
|
Division of Unemployment Insurance |
Document |
PO Box 9953 |
|
Wilmington, DE |
|
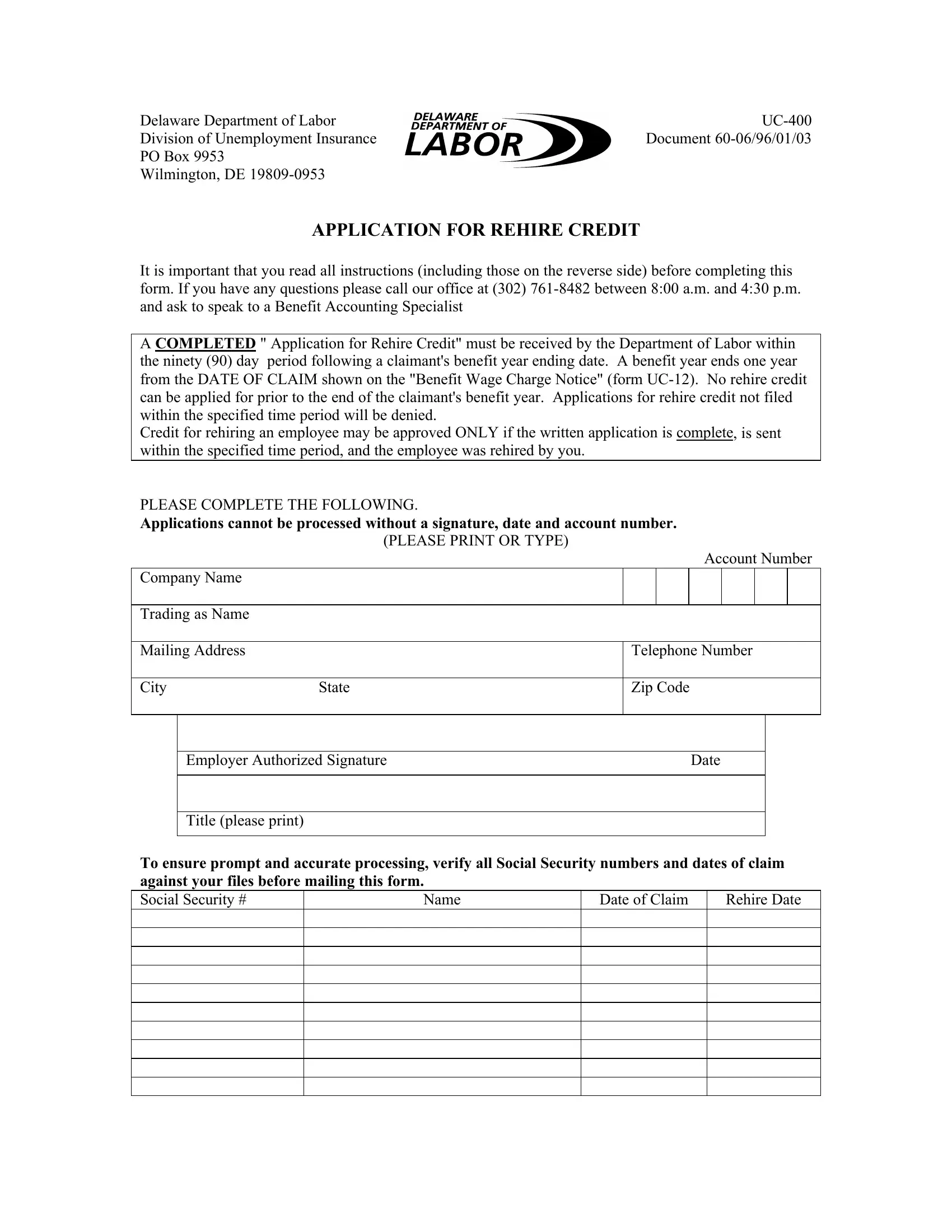
APPLICATION FOR REHIRE CREDIT
It is important that you read all instructions (including those on the reverse side) before completing this form. If you have any questions please call our office at (302)
A COMPLETED " Application for Rehire Credit" must be received by the Department of Labor within the ninety (90) day period following a claimant's benefit year ending date. A benefit year ends one year from the DATE OF CLAIM shown on the "Benefit Wage Charge Notice" (form
Credit for rehiring an employee may be approved ONLY if the written application is complete, is sent within the specified time period, and the employee was rehired by you.
PLEASE COMPLETE THE FOLLOWING.
Applications cannot be processed without a signature, date and account number.
|
|
(PLEASE PRINT OR TYPE) |
|
|
|
|
|
|
|
|
|
|
|
|
Account Number |
||||
Company Name |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Trading as Name |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
Mailing Address |
|
Telephone Number |
|||||||
|
|
|
|
|
|||||
City |
State |
Zip Code |
|||||||
|
|
|
|
|
|
||||
|
|
|
|
|
|
||||
|
Employer Authorized Signature |
|
|
Date |
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Title (please print) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
To ensure prompt and accurate processing, verify all Social Security numbers and dates of claim against your files before mailing this form.
Social Security # |
Name |
Date of Claim |
Rehire Date |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|