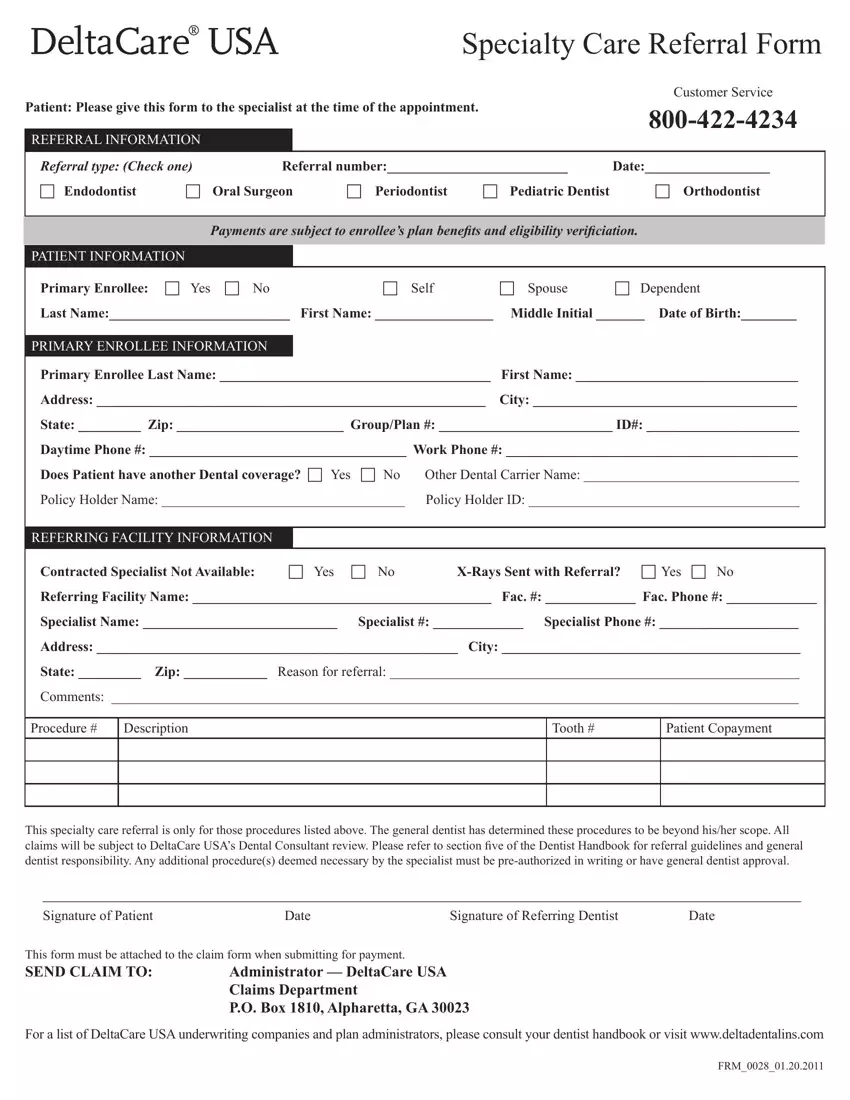
Specialty Care Referral Form
|
|
|
|
|
|
Customer Service |
Patient: Please give this form to the specialist at the time of the appointment. |
|
800-422-4234 |
|
|
|
|
|
|
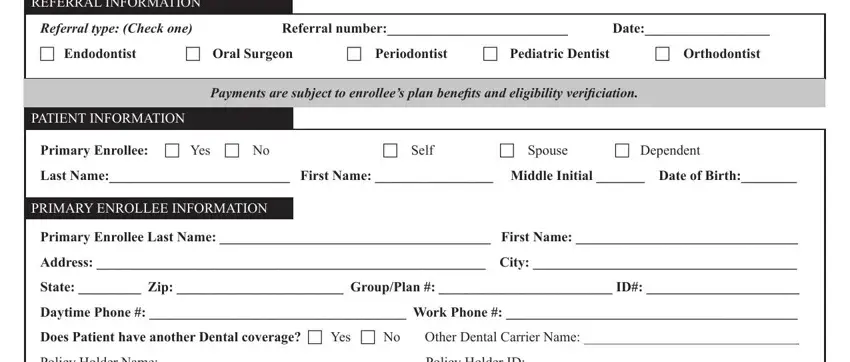
REFERRAL INFORMATION |
|
|
|
|
|
|
|
|
|
Referral type: (Check one) |
Referral number:__________________________ |
Date:__________________ |
c Endodontist |
c Oral Surgeon |
c Periodontist |
c Pediatric Dentist |
c Orthodontist |
|
|
|
|
|
|
|
Payments are subject to enrollee’s plan beneits and eligibility veriiciation.
PATIENT INFORMATION
Primary Enrollee: c Yes c No |
c Self |
c Spouse |
c Dependent |
Last Name:__________________________ |
First Name: _________________ |
Middle Initial _______ Date of Birth:________ |
|
|
|
|
PRIMARY ENROLLEE INFORMATION |
|
|
|
Primary Enrollee Last Name: _______________________________________ |
First Name: ________________________________ |
Address: ________________________________________________________ |
City: ______________________________________ |
State: _________ Zip: ________________________ Group/Plan #: _________________________ ID#: ______________________
Daytime Phone #: _____________________________________ Work Phone #: __________________________________________
Does Patient have another Dental coverage? c Yes |
c No |
Other Dental Carrier Name: _______________________________ |
Policy Holder Name: ___________________________________ |
Policy Holder ID: _______________________________________ |
|
|
|
|
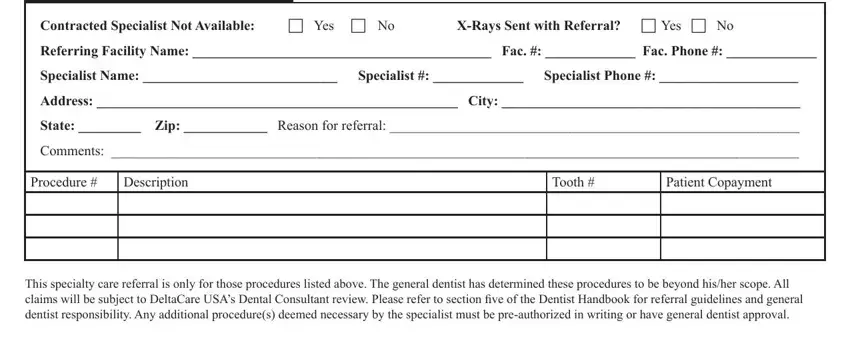
REFERRING FACILITY INFORMATION |
|
|
|
|
|
|
|
Contracted Specialist Not Available: |
c Yes |
c No |
X-Rays Sent with Referral? c Yes c No |
Referring Facility Name: ___________________________________________ Fac. #: _____________ Fac. Phone #: _____________
Specialist Name: ____________________________ Specialist #: _____________ Specialist Phone #: ____________________
Address: ____________________________________________________ City: ___________________________________________
State: _________ Zip: ____________ Reason for referral: ___________________________________________________________
Comments: ___________________________________________________________________________________________________
Procedure # |
Description |
Tooth # |
Patient Copayment |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
This specialty care referral is only for those procedures listed above. The general dentist has determined these procedures to be beyond his/her scope. All
claims will be subject to DeltaCare USA’s Dental Consultant review. Please refer to section ive of the Dentist Handbook for referral guidelines and general
dentist responsibility. Any additional procedure(s) deemed necessary by the specialist must be pre-authorized in writing or have general dentist approval.
___________________________________________________________________________________________
Signature of Patient |
Date |
Signature of Referring Dentist |
Date |
This form must be attached to the claim form when submitting for payment.
SEND CLAIM TO: |
Administrator — DeltaCare USA |
|
Claims Department |
|
P.O. Box 1810, Alpharetta, GA 30023 |
For a list of DeltaCare USA underwriting companies and plan administrators, please consult your dentist handbook or visit www.deltadentalins.com
FRM_0028_01.20.2011