The PDF editor was made to be as simple as possible. When you follow the next actions, the process of managing the deltacare referral form file will undoubtedly be simple.
Step 1: Press the button "Get form here" to open it.
Step 2: The document editing page is right now available. It's possible to add text or modify present content.
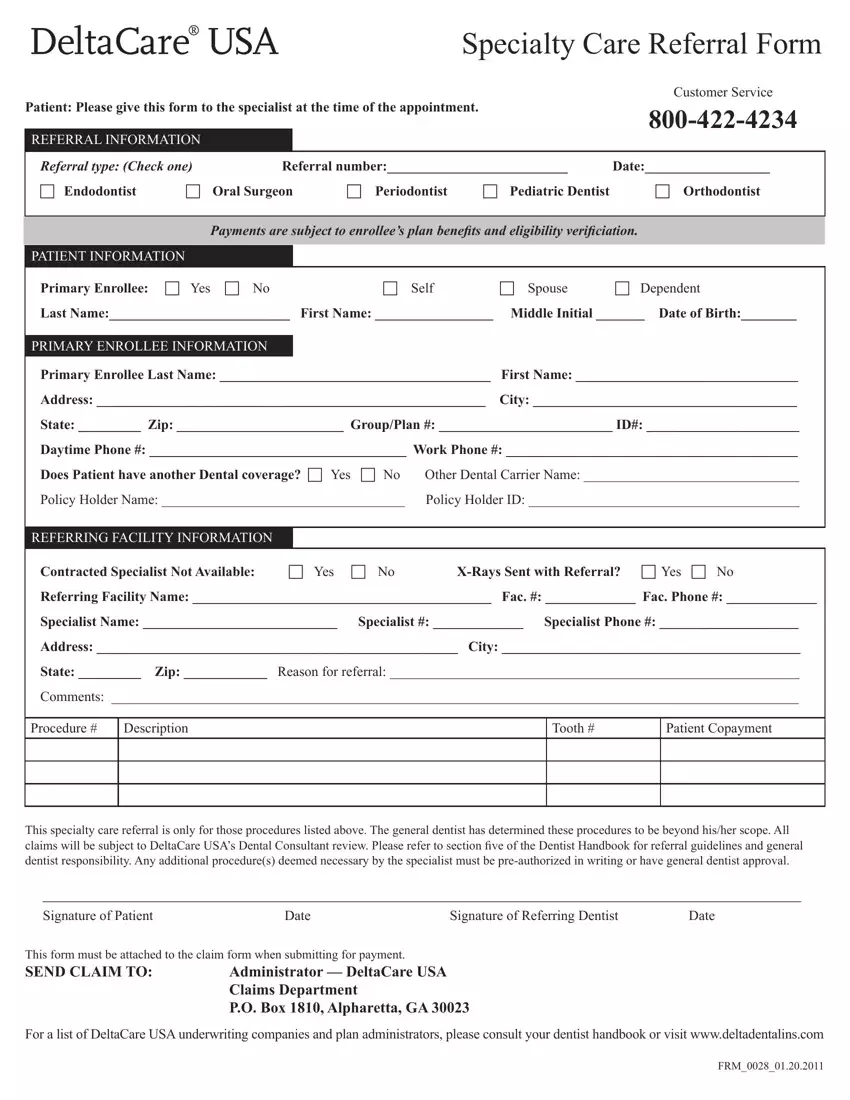
The PDF form you wish to complete will include the following segments:
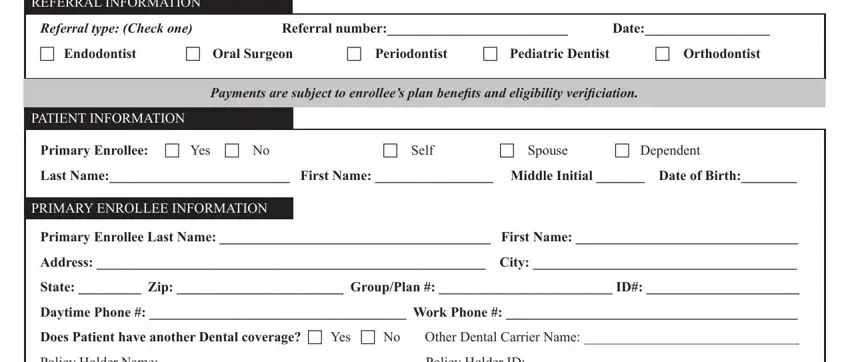
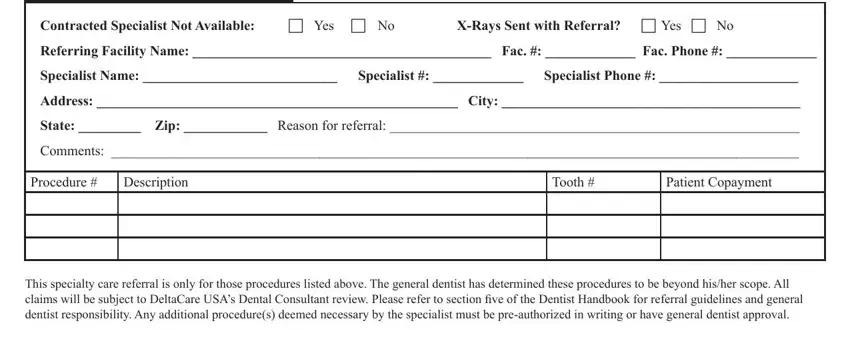
In the Contracted Specialist Not, XRays Sent with Referral c Yes c No, Referring Facility Name Fac Fac, Specialist Name Specialist, Address City, State Zip Reason for referral, Comments, Procedure, Description, Tooth, Patient Copayment, This specialty care referral is, and Signature of Patient box, jot down your details.
Step 3: Select the button "Done". Your PDF file is available to be exported. It's possible to upload it to your computer or email it.
Step 4: Produce a copy of every single document. It may save you time and enable you to remain away from misunderstandings down the road. Keep in mind, the information you have isn't distributed or checked by us.
