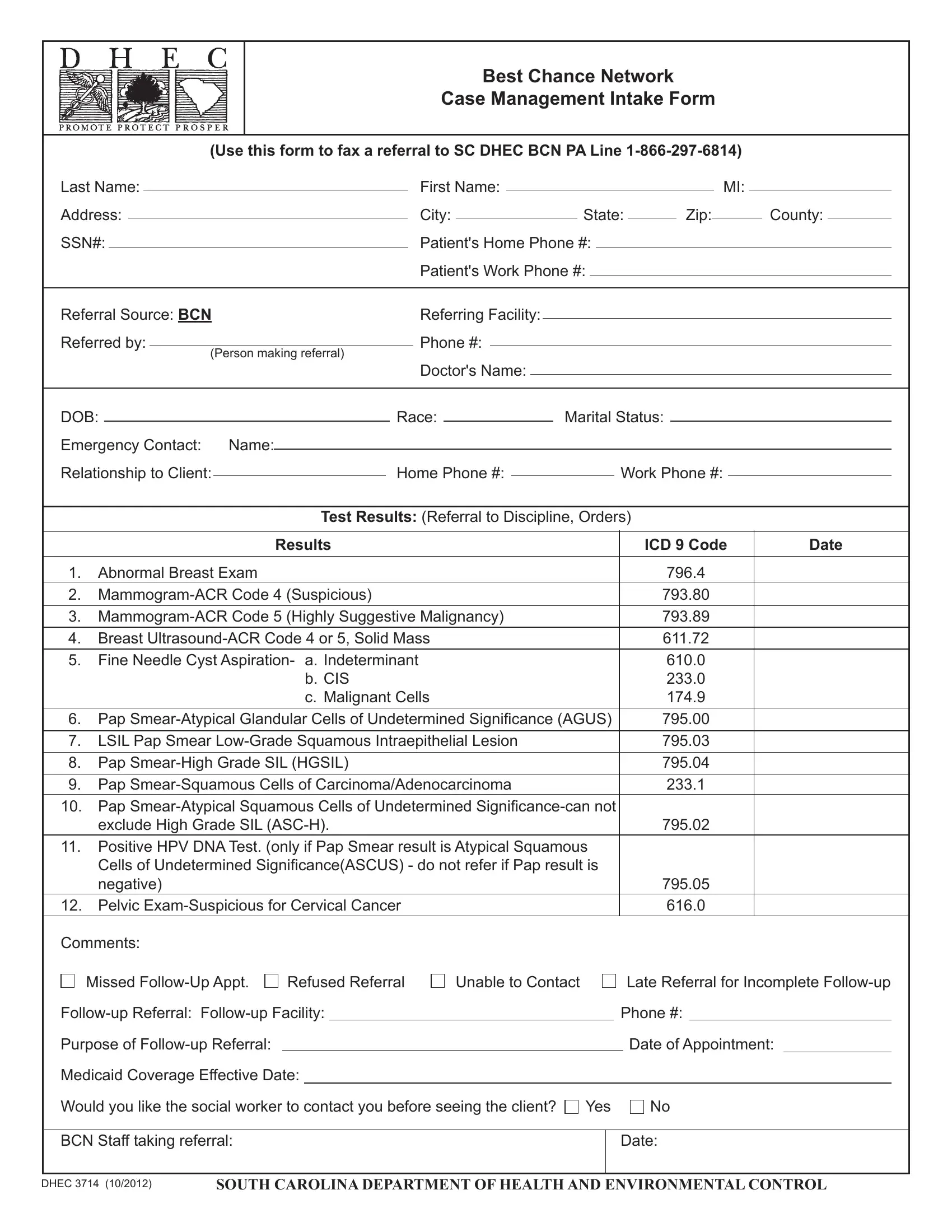
Designed as a critical component in South Carolina's health care system, the DHEC 3714 form serves a vital function in streamlining the referral process for the Best Chance Network (BCN) case management services. This detailed form encompasses various sections meant to provide comprehensive patient information, ranging from personal identifiers to medical test results, facilitating the referral pathway to BCN's specialized resources. The form is meticulously crafted to ensure a fluid exchange of information between referring facilities, such as physicians' offices, and the BCN staff. It prompts the referrer to supply essential data, including test results with specific ICD 9 codes, patient demographics, emergency contacts, and the necessity for follow-up referrals. Not only does it seek to bridge the referral gap but also aims to equip BCN case managers with all pertinent details needed to support the referred client effectively. Additionally, it outlines the procedural guidelines for filling out and submitting the form, specifying the distribution of copies to relevant parties to maintain a coherent communication channel. The DHEC 3714 form embodies a crucial administrative tool in fostering timely and efficient case management services under the BCN program, emphasizing the importance of detailed record-keeping and the collaborative efforts required to support patient needs adequately.
| Question | Answer |
|---|---|
| Form Name | Dhec 3714 Form |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | best chance network provider phone number, dhec best chance network, dhec south carolina best chance form 1382, best chance network |
Best Chance Network
Case Management Intake Form
(Use this form to fax a referral to SC DHEC BCN PA Line
Last Name: |
|
|
|
|
|
|
|
|
First Name: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
MI: |
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
Address: |
|
|
|
|
|
|
|
|
City: |
|
|
|
|
|
|
State: |
|
|
|
Zip: |
|
|
|
County: |
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
SSN#: |
|
|
|
|
|
|
|
|
Patient's Home Phone #: |
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
Patient's Work Phone #: |
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Referral Source: BCN |
|
|
|
|
Referring Facility: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
Referred by: |
|
|
|
|
|
|
|
Phone #: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
(Person making referral) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
Doctor's Name: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
DOB: |
|
|
|
|
|
Race: |
|
|
|
|
Marital Status: |
|
|
|
|
|
|
|||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||
Emergency Contact: Name: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
Relationship to Client: |
|
|
|
Home Phone #: |
|
|
|
|
|
|
|
Work Phone #: |
|
|
|
|
|
|||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Test Results: (Referral to Discipline, Orders) |
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Results |
|
|
|
|
|
|
|
ICD 9 Code |
|
Date |
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
1. |
Abnormal Breast Exam |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
796.4 |
|
|
|
|
|
|
|
|||||||||
2. |
|
|
|
|
|
|
|
793.80 |
|
|
|
|
|
|
|
|||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
3. |
|
|
|
|
|
|
|
793.89 |
|
|
|
|
|
|
|
|||||||||||||||||||||
4. |
Breast |
|
|
|
|
|
|
|
611.72 |
|
|
|
|
|
|
|
||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
5. |
Fine Needle Cyst Aspiration- |
a. Indeterminant |
|
|
|
|
|
|
|
610.0 |
|
|
|
|
|
|
|
|||||||||||||||||||
|
|
|
|
|
|
|
|
|
b. CIS |
|
|
|
|
|
|
|
233.0 |
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
c. Malignant Cells |
|
|
|
|
|
|
|
174.9 |
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
6. |
795.00 |
|
|
|
|
|
|
|
||||||||||||||||||||||||||||
7. |
LSIL Pap Smear |
|
|
|
|
|
|
|
795.03 |
|
|
|
|
|
|
|
||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
8. |
Pap |
|
|
|
|
|
|
|
795.04 |
|
|
|
|
|
|
|
||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
9. |
Pap |
|
|
|
|
|
|
|
233.1 |
|
|
|
|
|
|
|
||||||||||||||||||||
10. |
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||
|
exclude High Grade SIL |
|
|
|
|
|
|
|
795.02 |
|
|
|
|
|
|
|
||||||||||||||||||||
11.Positive HPV DNA Test. (only if Pap Smear result is Atypical Squamous
|
negative) |
|
|
|
|
|
|
795.05 |
|
|
||
|
12. Pelvic |
|
|
|
616.0 |
|
|
|||||
|
Comments: |
|
|
|
|
|
|
|
|
|
|
|
|
Missed |
Refused Referral |
Unable to Contact |
|
|
|
Late Referral for Incomplete |
|
||||
|
|
|
|
|
Phone #: |
|
|
|||||
|
Purpose of |
|
|
|
|
|
|
|
Date of Appointment: |
|
||
|
Medicaid Coverage Effective Date: |
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
||||
|
Would you like the social worker to contact you before seeing the client? |
Yes |
|
No |
|
|||||||
|
|
|
|
|
|
|
|
|
|
|||
|
BCN Staff taking referral: |
|
|
|
|
|
|
Date: |
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
DHEC 3714 (10/2012) |
SOUTH CAROLINA DEPARTMENT OF HEALTH AND ENVIRONMENTAL CONTROL |
Instructions for Completing the
Best Chance Network
Case Management Intake Form
DHEC 3714
Purpose: This form is to be used as an intake form for the BCN staff in order to complete a referral for BCN case man- agement services. The case managers will use the form for identifying the reason for the referral and to supply support- ive and identifying information. The appropriate district/county staff will also use the form for entering the BCN client in the Novius system.
Item by Item Instructions: In the irst box complete the identifying data for the BCN client being referred for case management services.
In the second box complete the blank for the referring facility (physician’s ofice), enter the name of the person faxing in the referral and the phone number where you can be reached.
In the third box complete the remaining identifying information as requested.
Test Results: Circle the number by the appropriate diagnosis and then give the date the test was completed.
Comments: Give additional information that might help the case manager in providing services for the client. Mark the appropriate box(s) for the items listed.
Medicaid Coverage Effective Date: Complete date that Medicaid is effective if known.
Mark the appropriate box, Yes or No, for request for social worker to contact the referring person prior to seeing the client.
Person Receiving Referral: The appropriate BCN staff receiving the referral needs to sign their name. All referrals must be signed by the staff who receives and processes the referral.
Date: Put the date that the referral was received and faxed to the social worker/case manager.
Ofice Mechanics and Filing: The original and three copies of this form are kept in different ofices. The BCN staff member keeps a copy in a notebook in their ofice. The Case Management program coordinator housed in Home Health keeps a copy in her ofice and the BCN Quality Management Coordinator keeps the original in the BCN ofice. Appropri-
ate personnel will keep all three of these under lock with limited access. These forms will have a retention schedule of
one year and should be shredded at the end of that year. A copy of the referral also goes to the appropriate district social worker/case manager. This form should be iled and retained in the clinical record in accordance with standards of the
Comprehensive Health Record User’s Manual and Home Health guidelines.
DHEC - 3714 (10/2012)