The State of Maryland-Child Protective Services Program employs the DHR SSA form as a critical tool for conducting background clearance and releasing information regarding child protective investigations. This meticulously structured document serves multiple essential purposes, chiefly among them, facilitating the release of pertinent information to individuals or entities undergoing a background check for roles directly impacting the welfare of children, such as foster care, adoption, or educational employment. The form demands thorough completion, including full identification details, current and past addresses, and family member information, ensuring a comprehensive search can be conducted. Additionally, it highlights the importance of notarization to verify the authenticity of the requester's identity and maintains the integrity of the process. The DHR SSA form acts as a gateway for individuals and agencies to access critical information about past child abuse or neglect findings, ensuring that children are placed in safe environments. It underscores the balance between the right to privacy and the paramount need for child safety within Maryland's legal framework, illustrating the state's commitment to child welfare through rigorous background checks.
| Question | Answer |
|---|---|
| Form Name | Dhr Ssa Form |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | how to maryland clearance, maryland tax clearance, dhr ssa, maryland release information |
State of
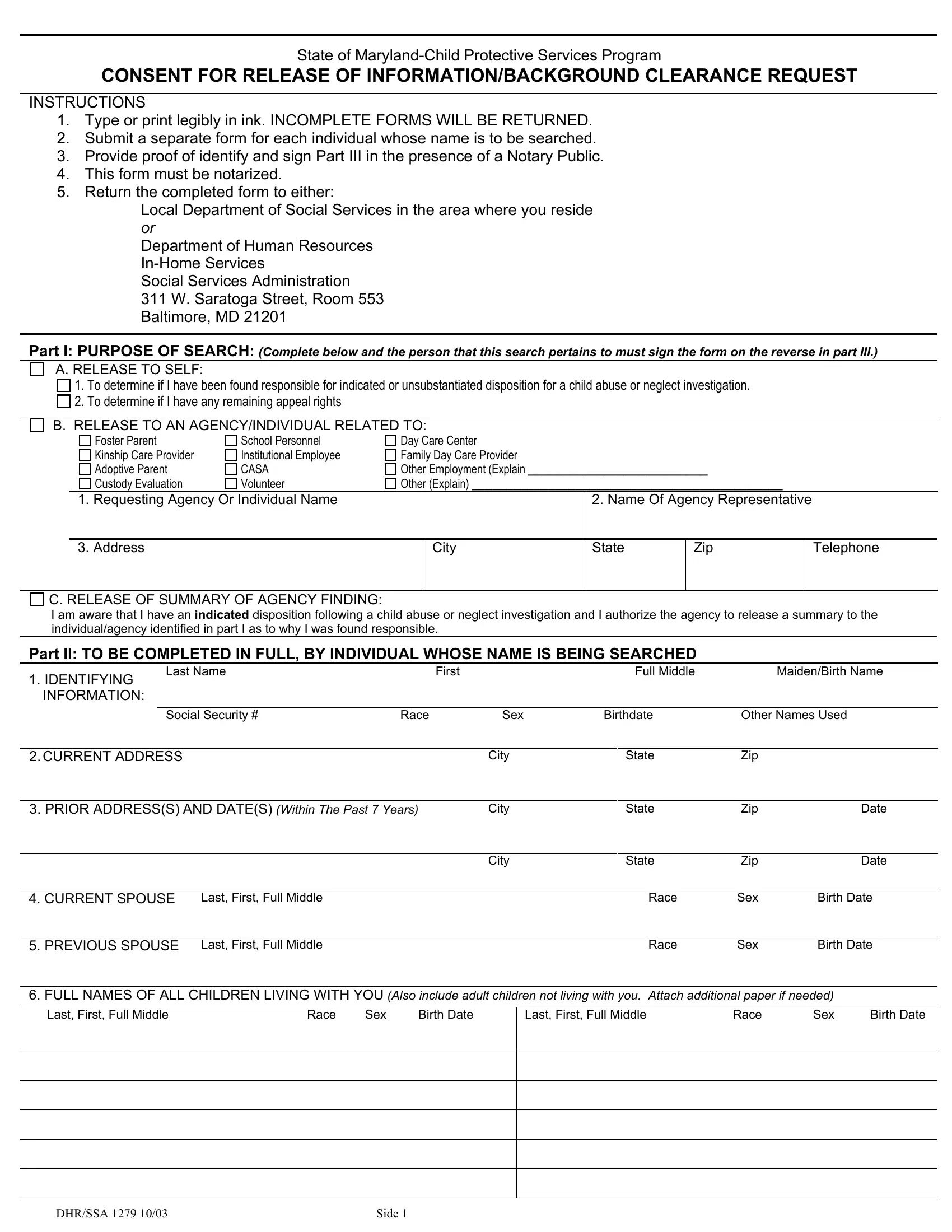
CONSENT FOR RELEASE OF INFORMATION/BACKGROUND CLEARANCE REQUEST
INSTRUCTIONS
1.Type or print legibly in ink. INCOMPLETE FORMS WILL BE RETURNED.
2.Submit a separate form for each individual whose name is to be searched.
3.Provide proof of identify and sign Part III in the presence of a Notary Public.
4.This form must be notarized.
5.Return the completed form to either:
Local Department of Social Services in the area where you reside or
Department of Human Resources
Social Services Administration
311 W. Saratoga Street, Room 553 Baltimore, MD 21201
PART I: PURPOSE OF SEARCH: (Complete below and the person that this search pertains to must sign the form on the reverse in part III.)
A. RELEASE TO SELF:
1. To determine if I have been found responsible for indicated or unsubstantiated disposition for a child abuse or neglect investigation.
2. To determine if I have any remaining appeal rights
B. RELEASE TO AN AGENCY/INDIVIDUAL RELATED TO:
Foster Parent
Kinship Care Provider
Adoptive Parent
Custody Evaluation
School Personnel
Institutional Employee
CASA
Volunteer
Day Care Center
Family Day Care Provider
Other Employment (Explain __________________________
Other (Explain) _____________________________________________
1. Requesting Agency Or Individual Name
2. Name Of Agency Representative
|
3. Address |
City |
State |
Zip |
Telephone |
|
|
|
|
|
|
C. RELEASE OF SUMMARY OF AGENCY FINDING:
I am aware that I have an INDICATED disposition following a child abuse or neglect investigation and I authorize the agency to release a summary to the individual/agency identified in part I as to why I was found responsible.
PART II: TO BE COMPLETED IN FULL, BY INDIVIDUAL WHOSE NAME IS BEING SEARCHED
1. IDENTIFYING |
Last Name |
|
First |
Full Middle |
|
Maiden/Birth Name |
|
|
|
|
|
|
|
|
|
INFORMATION: |
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
Social Security # |
Race |
Sex |
Birthdate |
Other Names Used |
||
|
|
|
|
|
|
|
|
2.CURRENT ADDRESS |
|
|
City |
State |
Zip |
|
|
|
|
|
|
|
|||
3. PRIOR ADDRESS(S) AND DATE(S) (Within The Past 7 Years) |
City |
State |
Zip |
Date |
|||
|
|
|
|
|
|
|
|
|
|
|
|
City |
State |
Zip |
Date |
|
|
|
|
|
|
|
|
4. CURRENT SPOUSE |
Last, First, Full Middle |
|
|
Race |
Sex |
Birth Date |
|
|
|
|
|
|
|
|
|
5. PREVIOUS SPOUSE |
Last, First, Full Middle |
|
|
Race |
Sex |
Birth Date |
|
6.FULL NAMES OF ALL CHILDREN LIVING WITH YOU (Also include adult children not living with you. Attach additional paper if needed)
Last, First, Full Middle |
Race |
Sex |
Birth Date |
Last, First, Full Middle |
Race |
Sex |
Birth Date |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DHR/SSA 1279 10/03 |
SIDE 1 |
PART III: AUTHORIZATION (Check either 1 or 2 below. )
Pursuant to Maryland Code of Regulation Section 07.02.07.19, pertaining to the confidentiality of Child Protective Services records and reports, I hereby authorize the Maryland Department of Human Resources (DHR):
1. To notify _______________________________ (self, agency, or individual listed in part I) as to whether a local department of
social services has identified me as responsible for “indicated” child abuse or neglect in any record maintained by the Maryland DHR, any Local Department of Social Services, and Child Protective Services.
2. To release a summary of the indicated finding to _____________________________(self, agency, or individual listed in part I).
SIGNATURE: This form must sign in the presence of a Notary Public by the person named in part II. DATE:
PART IV. CERTIFICATE OF ACKNOWLEDGEMENT OF INDIVIDUAL BEFORE A NOTARY PUBLIC
City/County of: _______________________________________________ State of: _______________________________
Acknowledged before me this ____________________________ Day of _______________________ 20____
Notary Public
My Commission expires: ______________________
PART V. BACKGROUND CLEARANCE FINDINGS (for Local Department or DHR use only)
1.We are unable to determine at this time if the individual for whom a search has been requested has a CPS finding. Form returned to requesting agency. Date ____________
|
2. Sent to DHR or Local Department of Social Services: |
|
Name ______________________________________________ |
|
|
|
|
||
|
|
|
Date ________________ |
|
|
|
|
Date returned from Local Department _______________________ |
|
|
3. |
Based on information provided by Local Departments of Social Services, we have determined that __________________________ is listed in the |
|
||||||
|
|
Central Registry as being responsible for an |
Indicated/ |
Unsubstantiated disposition of |
Abuse / |
Neglect in reference to an |
|
||
|
|
investigation conducted in ______________________________. Child Protective Service Case/File/Referral #: ___________________________. |
|
||||||
|
4. |
Holding for Appeal |
|
Appeal Date ___________________________ Appeal Disposition __________________________________ |
|
||||
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
5.Notification sent to Requesting Agency/Individual: Date______________________________
6.Notification sent to Person: Date______________________________
7.Summary Provided: Date __________________________________
8.As of this date, the individual whose name was being searched is NOT identified in the Central Registry as being responsible for abuse or neglect.
DHR/SSA 1279 10/03 |
SIDE 2 |