
When working in the online editor for PDFs by FormsPal, it is easy to complete or modify dma3051 here. In order to make our editor better and more convenient to utilize, we constantly work on new features, with our users' feedback in mind. Here is what you'll need to do to begin:
Step 1: Open the PDF form in our editor by clicking on the "Get Form Button" above on this page.
Step 2: The editor helps you work with your PDF form in a range of ways. Improve it by adding your own text, correct original content, and put in a signature - all at your disposal!
It is easy to finish the document using out detailed tutorial! This is what you should do:
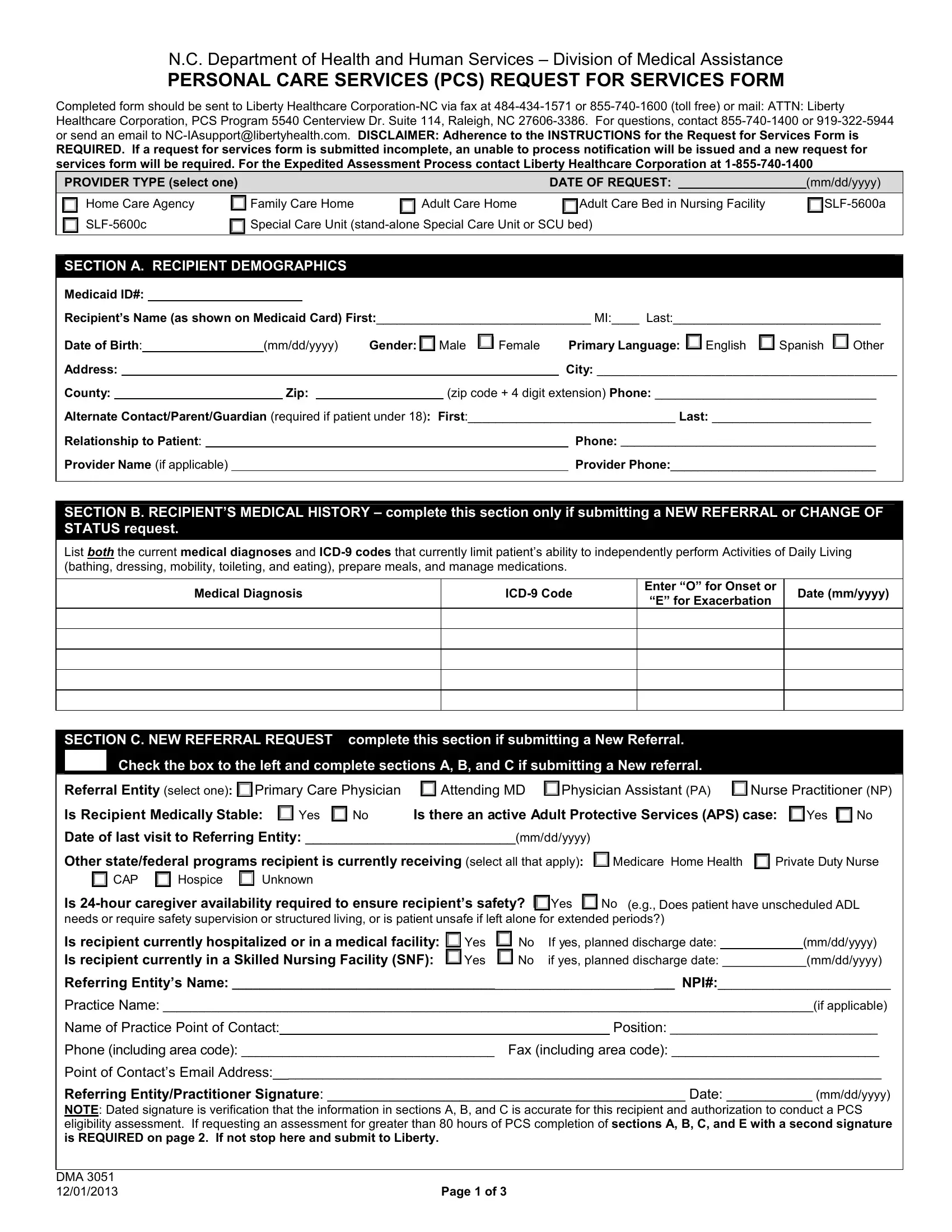
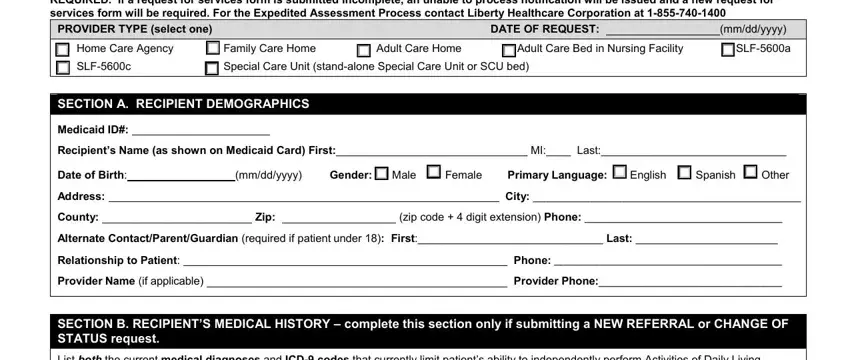
1. The dma3051 usually requires particular details to be typed in. Ensure the next blanks are filled out:
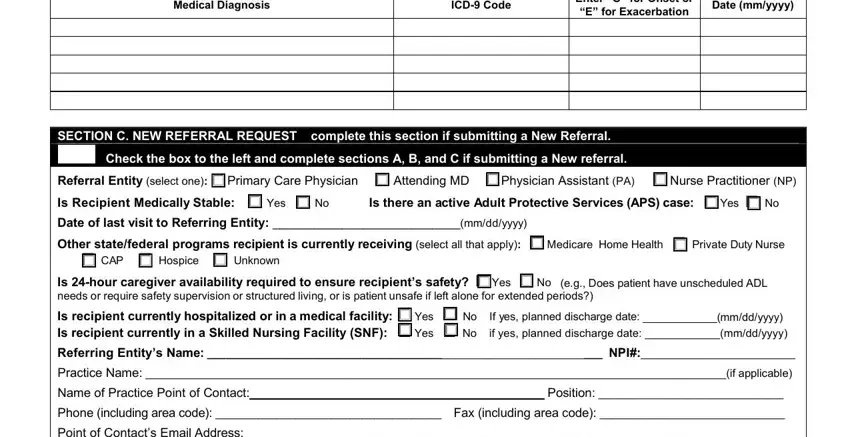
2. The subsequent part is to fill in all of the following blank fields: Medical Diagnosis, ICD Code, Date mmyyyy, Enter O for Onset or E for, SECTION C NEW REFERRAL REQUEST, Check the box to the left and, Referral Entity select one cid, Date of last visit to Referring, cid CAP cid Hospice cid Unknown, Is hour caregiver availability, Referring Entitys Name NPI, Practice Name if applicable, Name of Practice Point of Contact, Position, and Phone including area code Fax.
3. Completing Point of Contacts Email Address, DMA, and Page of is essential for the next step, make sure to fill them out in their entirety. Don't miss any details!

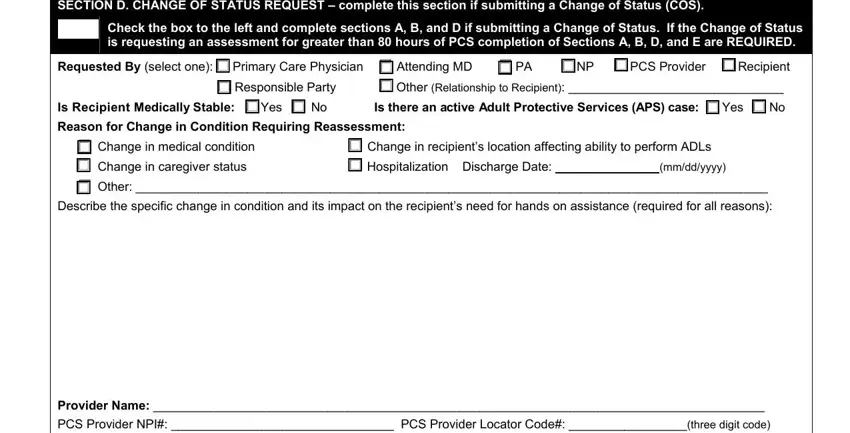
4. Your next part will require your attention in the subsequent areas: SECTION D CHANGE OF STATUS REQUEST, Check the box to the left and, Requested By select one cid, cid Change in medical condition, mmddyyyy, Provider Name, and PCS Provider NPI PCS Provider. Make certain you fill in all required details to go further.
It is easy to make errors when filling out the mmddyyyy, consequently make sure to look again before you decide to finalize the form.
5. Because you approach the conclusion of this form, you'll notice several more things to undertake. Mainly, Facility License if applicable, Provider Contact Name Contacts, Practice Phone Practice Fax, Email, Referring EntityPractitioner, Practitioner First Name Last Name, Practice Name if applicable, Practice Contacts Name Contacts, Practice Phone Practice Fax, Email, SECTION E PHYSICIAN ATTESTATION, The recipient requires an, The recipient requires caregivers, characterized by irreversible, and Regardless of setting the must all be filled out.
Step 3: After going through the fields, click "Done" and you are done and dusted! Right after getting a7-day free trial account here, you will be able to download dma3051 or send it via email right off. The PDF document will also be available via your personal account menu with all your adjustments. FormsPal is committed to the confidentiality of our users; we make sure all personal information coming through our editor remains confidential.