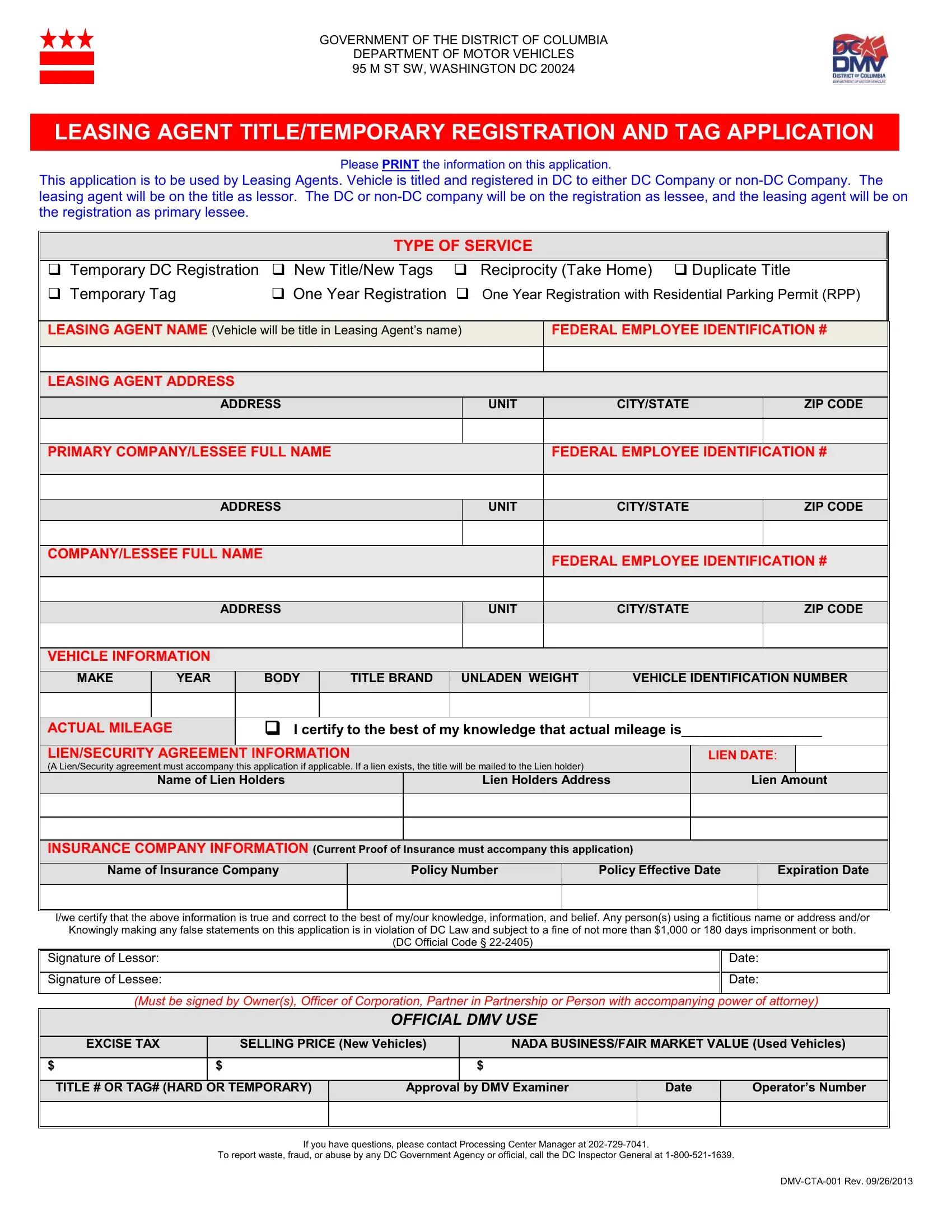
Navigating the intricacies of vehicle leasing and registration in Washington, D.C., requires meticulous attention to detail and adherence to specific procedures as set forth by the Department of Motor Vehicles (DMV). One of the primary tools in this process is the DMV CTA 001 form, a crucial document for leasing agents operating within the district. This form serves multiple functions, including the application for a new title, temporary or one-year registration tags, and the necessary permissions for reciprocal vehicle use. Specifically designed for leasing agents, the form mandates the inclusion of both the agent's and the lessee's information, detailing their names, addresses, and Federal Employee Identification Numbers, alongside the vehicle’s specifics such as make, year, body type, and Vehicle Identification Number (VIN). Additionally, it addresses the need for a lien/security agreement if applicable, ensuring the title is mailed to the correct lienholder, and mandates current proof of insurance. The DMV CTA 001 form encapsulates a critical interface between leasing companies, lessees, and the government, establishing a structured pathway for legal vehicle leasing, titling, and registration, further emphasizing the importance of accuracy and honesty in providing the required information to avoid legal penalties for falsification. Its comprehensive nature ensures that all parties are adequately protected and that the vehicle can lawfully be operated within the district, highlighting its indispensable role in the regulatory framework that governs vehicle leasing in the District of Columbia.
| Question | Answer |
|---|---|
| Form Name | Dmv Cta 001 Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | cta 001, dmv title temporary, dmv cta 001 washington dc, southwest service center |
GOVERNMENT OF THE DISTRICT OF COLUMBIA
DEPARTMENT OF MOTOR VEHICLES
95 M ST SW, WASHINGTON DC 20024
LEASING AGENT TITLE/TEMPORARY REGISTRATION AND TAG APPLICATION
Please PRINT the information on this application.
This application is to be used by Leasing Agents. Vehicle is titled and registered in DC to either DC Company or
TYPE OF SERVICE
|
Temporary DC Registration |
New Title/New Tags |
Reciprocity (Take Home) Duplicate Title |
|||||||||||||||||||||
|
Temporary Tag |
|
|
One Year Registration |
One Year Registration with Residential Parking Permit (RPP) |
|||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
LEASING AGENT NAME (Vehicle will be title in Leasing Agent’s name) |
|
FEDERAL EMPLOYEE IDENTIFICATION # |
|
||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
LEASING AGENT ADDRESS |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
ADDRESS |
|
|
|
|
UNIT |
|
|
|
|
CITY/STATE |
|
|
|
|
ZIP CODE |
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
PRIMARY COMPANY/LESSEE FULL NAME |
|
|
|
|
|
|
FEDERAL EMPLOYEE IDENTIFICATION # |
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
ADDRESS |
|
|
|
|
UNIT |
|
|
|
|
CITY/STATE |
|
|
|
|
ZIP CODE |
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
COMPANY/LESSEE FULL NAME |
|
|
|
|
|
|
|
|
FEDERAL EMPLOYEE IDENTIFICATION # |
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
ADDRESS |
|
|
|
|
UNIT |
|
|
|
|
CITY/STATE |
|
|
|
|
ZIP CODE |
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
VEHICLE INFORMATION |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
MAKE |
|
YEAR |
|
BODY |
|
TITLE BRAND |
UNLADEN WEIGHT |
|
VEHICLE IDENTIFICATION NUMBER |
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
ACTUAL MILEAGE |
|
|
I certify to the best of my knowledge that actual mileage is__________________ |
||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
LIEN/SECURITY AGREEMENT INFORMATION |
|
|
|
|
|
|
|
|
|
|
|
LIEN DATE: |
|
|
|||||||||
|
(A Lien/Security agreement must accompany this application if applicable. If a lien exists, the title will be mailed to the Lien holder) |
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
Name of Lien Holders |
|
|
|
|
Lien Holders Address |
|
|
Lien Amount |
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
INSURANCE COMPANY INFORMATION (Current Proof of Insurance must accompany this application) |
|
|
|
|
|
|
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
Name of Insurance Company |
|
Policy Number |
|
|
|
|
Policy Effective Date |
|
|
Expiration Date |
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
I/we certify that the above information is true and correct to the best of my/our knowledge, information, and belief. Any person(s) using a fictitious name or address and/or Knowingly making any false statements on this application is in violation of DC Law and subject to a fine of not more than $1,000 or 180 days imprisonment or both.
(DC Official Code §
Signature of Lessor:
Signature of Lessee:
Date:
Date:
(Must be signed by Owner(s), Officer of Corporation, Partner in Partnership or Person with accompanying power of attorney)
OFFICIAL DMV USE
|
EXCISE TAX |
|
|
SELLING PRICE (New Vehicles) |
|
|
NADA BUSINESS/FAIR MARKET VALUE (Used Vehicle |
s) |
|
||||||
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
$ |
|
$ |
|
|
|
$ |
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|||||
|
TITLE # OR TAG# (HARD OR TEMPORARY) |
|
Approval by DMV Examiner |
|
Date |
|
Operator’s Number |
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
If you have questions, please contact Processing Center Manager at
To report waste, fraud, or abuse by any DC Government Agency or official, call the DC Inspector General at