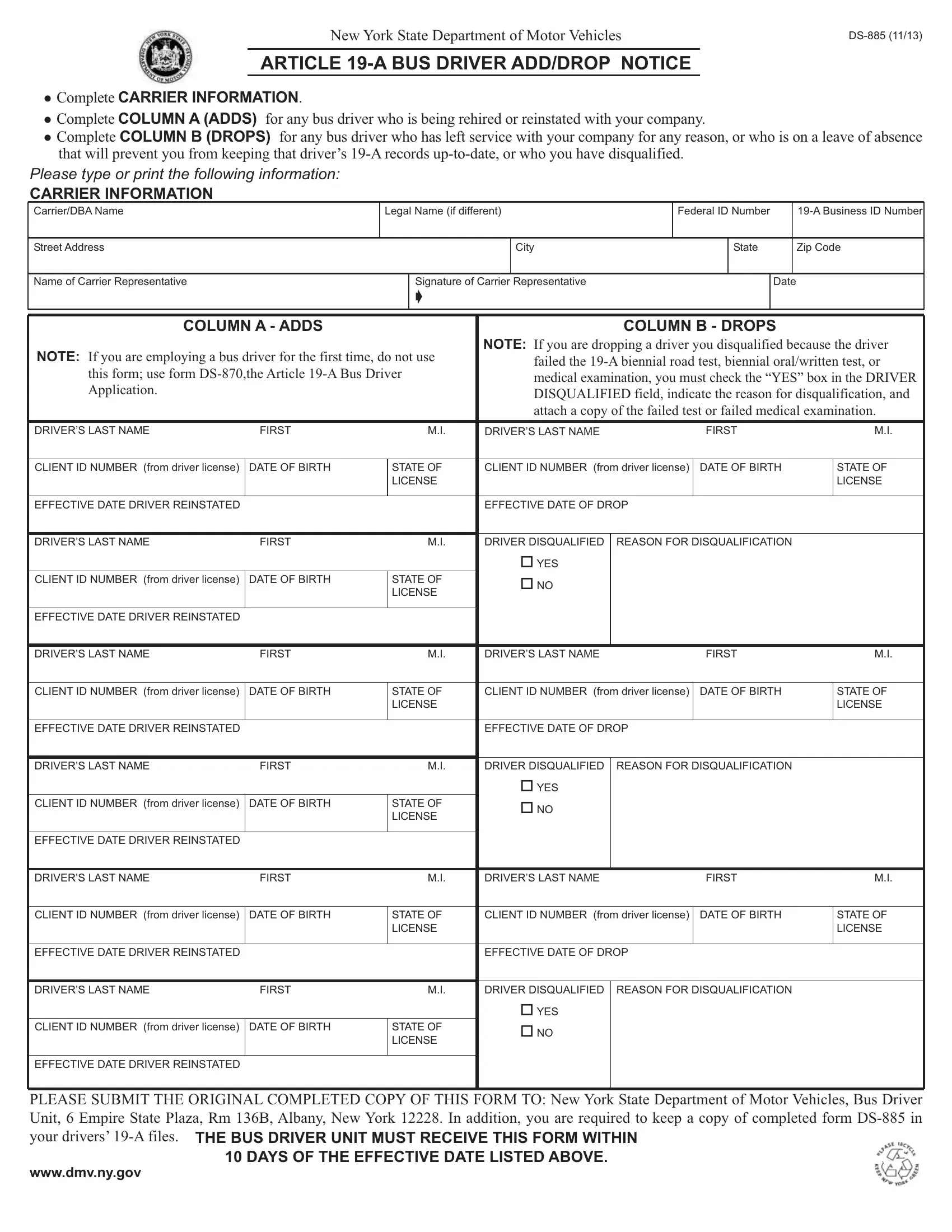
Understanding the complexities and requirements of the DMV DS 885 form is crucial for transportation companies and those in charge of managing bus drivers. This form serves as a vital tool for reporting significant changes in the status of bus drivers to the New York State Department of Motor Vehicles. Whether bus drivers are being added to a company's roster due to hiring, rehiring, or reinstatement, or being dropped because of resignation, leave of absence, or disqualification, accurate completion and timely submission of this form is required. Specifically, the form mandates that the bus driver unit receives it within 10 days of any change in a driver's employment status. Detailed sections for both additions and removals of drivers ensure that companies can maintain up-to-date records and comply with Article 19-A, which aims to ensure the safety and reliability of bus drivers. By providing spaces for carrier information, driver details, and specific reasons for disqualification when applicable, the form also instructs carriers to include necessary documentation for drivers who fail required tests or medical examinations. The requirement to submit this form to the New York State Department of Motor Vehicles, along with keeping a copy in the driver's 19-A file, underscores the importance of this document in managing the qualifications and eligibility of bus drivers responsibly.
| Question | Answer |
|---|---|
| Form Name | Dmv Form Ds 885 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | 220C, disqualification, rehired, DS-885 |

NewYorkStateDepartmentofMotorVehicles
ARTICLE
CompleteCARRIERINFORMATION.
CompleteCOLUMNA(ADDS) foranybusdriverwhoisbeingrehiredorreinstatedwithyourcompany.
CompleteCOLUMNB(DROPS) foranybusdriverwhohasleftservicewithyourcompanyforanyreason,orwhoisonaleaveofabsence
Pleasetypeorprintthefollowinginformation:
CARRIER INFORMATION
Carrier/DBAName |
|
Legal Name (if different) |
|
Federal ID Number |
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
StreetAddress |
|
|
|
|
|
City |
|
|
|
State |
|
Zip Code |
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Name of Carrier Representative |
|
|
|
Signature of Carrier Representative |
|
|
|
|
Date |
|
|
|||
|
|
|
ç |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
COLUMN B - DROPS |
|
|
|||||||
NOTE: Ifyouare employingabusdriverforthefirsttime,donotuse |
NOTE: Ifyouare droppinga driveryoudisqualifiedbecause thedriver |
|||||||||||||
|
failedthe |
|||||||||||||
thisform;use form |
|
|||||||||||||
|
medicalexamination,youmustcheckthe“YES”boxintheDRIVER |
|||||||||||||
Application. |
|
|
|
|
|
|||||||||
|
|
|
|
|
DISQUALIFIEDfield,indicatethe reasonfordisqualification,and |
|||||||||
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
attachacopyofthefailedtestorfailedmedicalexamination. |
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DRIVER’S LAST NAME |
FIRST |
|
|
M.I. |
DRIVER’S LAST NAME |
|
|
FIRST |
|
M.I. |
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CLIENT ID NUMBER (from driver license) |
DATE OF BIRTH |
|
STATEOF |
CLIENT ID NUMBER (from driver license) |
DATE OF BIRTH |
|
STATEOF |
|||||||
|
|
|
LICENSE |
|
|
|
|
|
|
|
|
|
LICENSE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
EFFECTIVE DATE DRIVER REINSTATED |
|
|
|
|
EFFECTIVE DATE OF DROP |
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DRIVER’S LAST NAME |
FIRST |
|
|
M.I. |
DRIVER DISQUALIFIED |
REASON FOR DISQUALIFICATION |
|
|
||||||
|
|
|
|
|
|
oYES |
|
|
|
|
|
|
|
|
CLIENT ID NUMBER (from driver license) |
DATE OF BIRTH |
|
STATEOF |
|
oNO |
|
|
|
|
|
|
|
|
|
|
|
|
LICENSE |
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
EFFECTIVE DATE DRIVER REINSTATED |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DRIVER’S LAST NAME |
FIRST |
|
|
M.I. |
DRIVER’S LAST NAME |
|
|
FIRST |
|
M.I. |
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CLIENT ID NUMBER (from driver license) |
DATE OF BIRTH |
|
STATEOF |
CLIENT ID NUMBER (from driver license) |
DATE OF BIRTH |
|
STATEOF |
|||||||
|
|
|
LICENSE |
|
|
|
|
|
|
|
|
|
LICENSE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
EFFECTIVE DATE DRIVER REINSTATED |
|
|
|
|
EFFECTIVE DATE OF DROP |
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DRIVER’S LAST NAME |
FIRST |
|
|
M.I. |
DRIVER DISQUALIFIED |
REASON FOR DISQUALIFICATION |
|
|
||||||
|
|
|
|
|
|
oYES |
|
|
|
|
|
|
|
|
CLIENT ID NUMBER (from driver license) |
DATE OF BIRTH |
|
STATEOF |
|
oNO |
|
|
|
|
|
|
|
|
|
|
|
|
LICENSE |
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
EFFECTIVE DATE DRIVER REINSTATED |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DRIVER’S LAST NAME |
FIRST |
|
|
M.I. |
DRIVER’S LAST NAME |
|
|
FIRST |
|
M.I. |
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CLIENT ID NUMBER (from driver license) |
DATE OF BIRTH |
|
STATEOF |
CLIENT ID NUMBER (from driver license) |
DATE OF BIRTH |
|
STATEOF |
|||||||
|
|
|
LICENSE |
|
|
|
|
|
|
|
|
|
LICENSE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
EFFECTIVE DATE DRIVER REINSTATED |
|
|
|
|
EFFECTIVE DATE OF DROP |
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DRIVER’S LAST NAME |
FIRST |
|
|
M.I. |
DRIVER DISQUALIFIED |
REASON FOR DISQUALIFICATION |
|
|
||||||
|
|
|
|
|
|
oYES |
|
|
|
|
|
|
|
|
CLIENT ID NUMBER (from driver license) |
DATE OF BIRTH |
|
STATEOF |
|
oNO |
|
|
|
|
|
|
|
|
|
|
|
|
LICENSE |
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
EFFECTIVE DATE DRIVER REINSTATED |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PLEASE SUBMITTHE ORIGINALCOMPLETED COPYOF THIS FORM TO: NewYork State Department of Motor Vehicles, Bus Driver Unit, 6 Empire State Plaza, Rm 136B, Albany, New York 12228. In addition, you are required to keep a copy of completed form
www.dmv.ny.gov