

You could fill in vision test dmv illinois instantly using our online tool for PDF editing. We are dedicated to providing you with the perfect experience with our tool by constantly introducing new features and enhancements. With these updates, working with our editor gets easier than ever! Starting is easy! All you need to do is adhere to the following simple steps directly below:
Step 1: Firstly, open the pdf editor by clicking the "Get Form Button" in the top section of this webpage.
Step 2: After you start the editor, there'll be the document prepared to be filled out. Aside from filling out various blanks, you may as well do some other things with the PDF, such as writing your own textual content, editing the original text, adding illustrations or photos, putting your signature on the document, and much more.
Filling out this document needs thoroughness. Make sure that all mandatory blank fields are filled out properly.
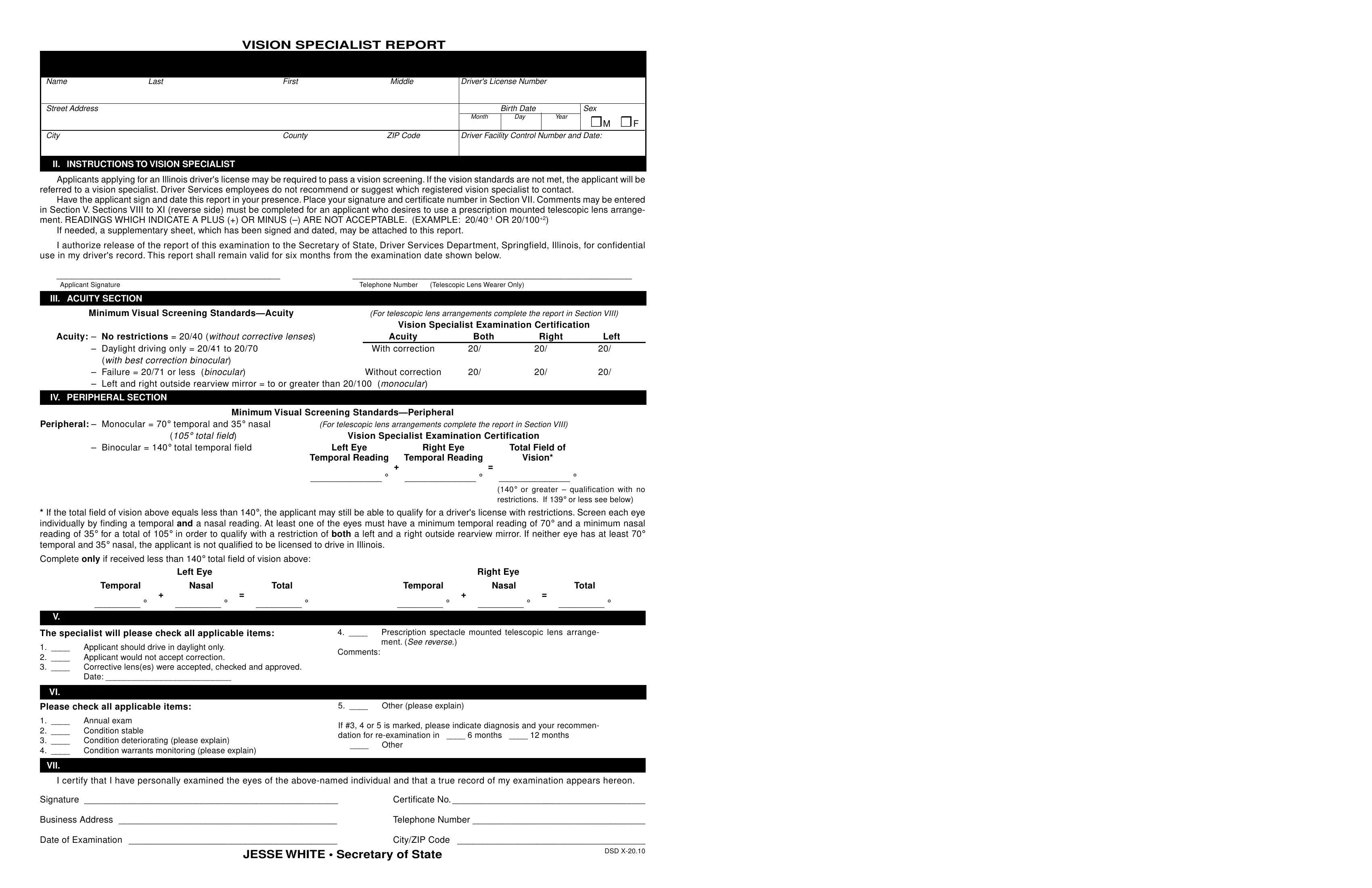
1. The vision test dmv illinois involves certain details to be entered. Ensure the next fields are finalized:
2. The next step would be to fill out these fields: Binocular total temporal field, Left Eye, Right Eye, Temporal Reading, Temporal Reading, Total Field of, Vision, or greater qualification with, If the total field of vision, Temporal, Left Eye, Nasal, Total, Temporal, and Right Eye.
3. This next step is related to I certify that I have personally, Signature, Certificate No, Business Address, Telephone Number, Date of Examination, JESSE WHITE Secretary of State, and CityZIP Code DSD X - fill in each one of these blanks.

4. To move onward, this fourth stage requires completing a few blanks. These comprise of Prescription Spectacle Mounted, Telescopic lenses may not exceed, monocular vision through, IX PERIPHERAL SECTION, Acuity, Both, Right, Left, Through carrier lenses Through, Minimum Visual Screening, Prescription Spectacle Mounted, Peripheral binocular or, spectacle mounted telescopic, Vision Specialist Examination, and Left Eye, which you'll find vital to moving forward with this particular PDF.
5. To wrap up your form, this last part requires some additional blank fields. Completing Date the applicant received the, Power of the telescopic lens, Is the patients condition stable, In your professional opinion is, may not be capable of safely, Indicate any additional comments, Yes, Yes, Has the patient successfully, The patient has been fitted for a, for at least days prior to the, The patient has clinically, telescopic lens and moving the, The patient has clinically, and the head and eyes in a coordinated should conclude everything and you'll be done in the blink of an eye!
As to Has the patient successfully and The patient has clinically, ensure you get them right in this current part. Both of these are the most important fields in the form.
Step 3: Before obtaining the next stage, make sure that all blank fields were filled in the correct way. When you determine that it's good, click “Done." Create a 7-day free trial account at FormsPal and obtain direct access to vision test dmv illinois - readily available inside your personal account. At FormsPal.com, we strive to guarantee that all your information is kept secure.