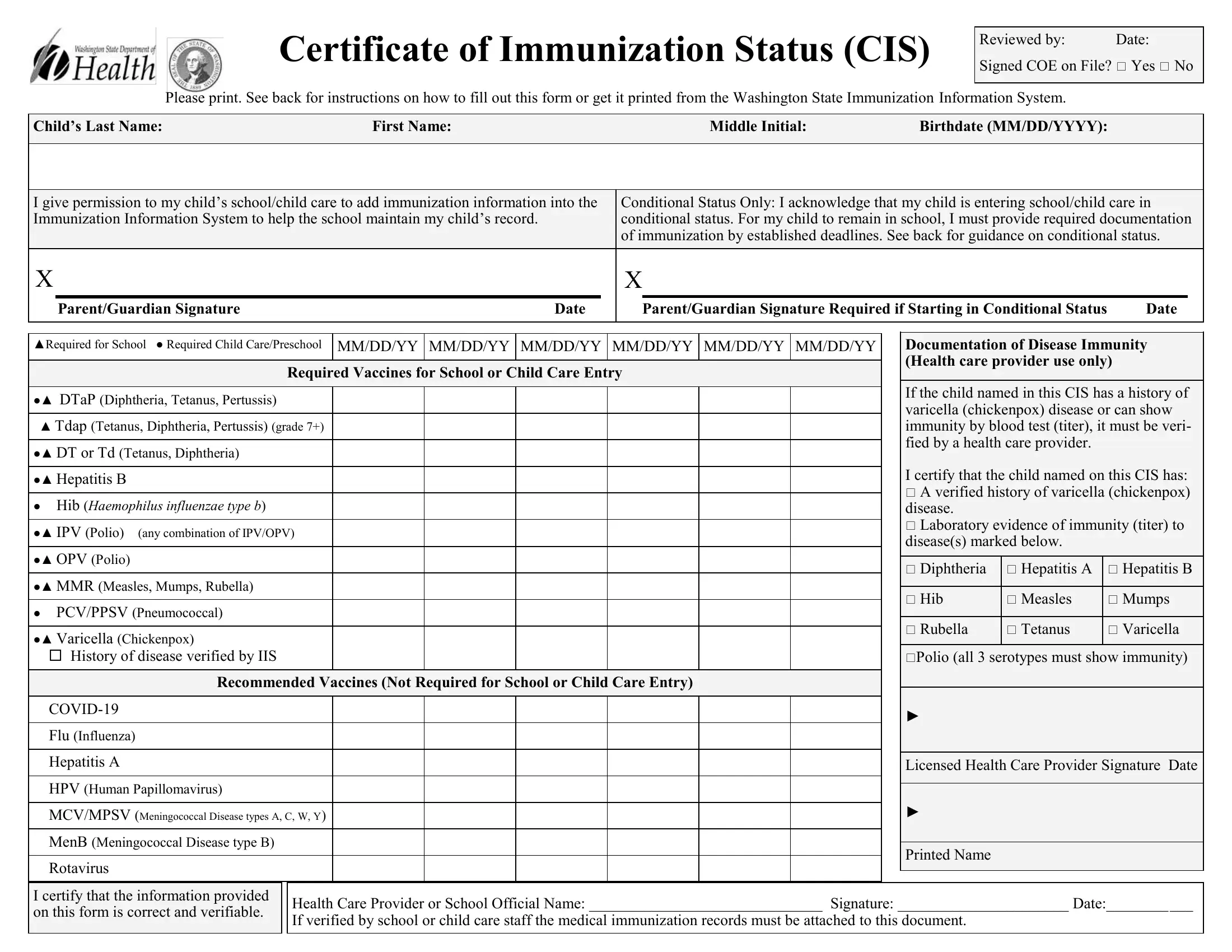
Certificate of Immunization Status (CIS)
Reviewed by: Date:
Signed COE on File? Yes No
Please print. See back for instructions on how to fill out this form or get it printed from the Washington State Immunization Information System.
Child’s Last Name: |
First Name: |
|
Middle Initial: |
Birthdate (MM/DD/YYYY): |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
I give permission to my child’s school/child care to add immunization information into the |
Conditional Status Only: I acknowledge that my child is entering school/child care in |
Immunization Information System to help the school maintain my child’s record. |
conditional status. For my child to remain in school, I must provide required documentation |
|
|
|
|
of immunization by established deadlines. See back for guidance on conditional status. |
X |
|
|
X |
|
|
|
|
Parent/Guardian Signature |
Date |
|
|
Parent/Guardian Signature Required if Starting in Conditional Status |
Date |
|
|
|
|
|
|
|
|
|
|
▲Required for School ● Required Child Care/Preschool MM/DD/YY MM/DD/YY MM/DD/YY MM/DD/YY MM/DD/YY MM/DD/YY
Required Vaccines for School or Child Care Entry
●▲ DTaP (Diphtheria, Tetanus, Pertussis)
▲Tdap (Tetanus, Diphtheria, Pertussis) (grade 7+) ●▲ DT or Td (Tetanus, Diphtheria)
●▲ Hepatitis B
●Hib (Haemophilus influenzae type b)
●▲ IPV (Polio) (any combination of IPV/OPV)
●▲ OPV (Polio)
●▲ MMR (Measles, Mumps, Rubella)
●PCV/PPSV (Pneumococcal)
●▲ Varicella (Chickenpox)
History of disease verified by IIS
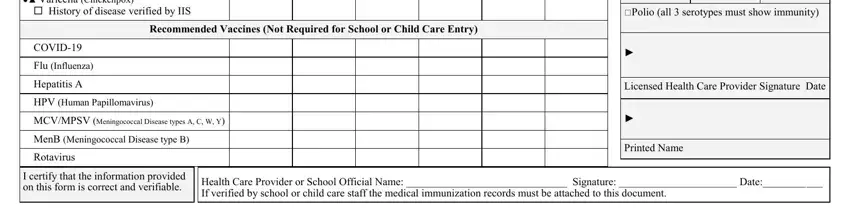
Recommended Vaccines (Not Required for School or Child Care Entry)
COVID-19
Flu (Influenza)
Hepatitis A
HPV (Human Papillomavirus)
MCV/MPSV (Meningococcal Disease types A, C, W, Y)
MenB (Meningococcal Disease type B)
Rotavirus
Documentation of Disease Immunity (Health care provider use only)
If the child named in this CIS has a history of varicella (chickenpox) disease or can show immunity by blood test (titer), it must be veri- fied by a health care provider.
I certify that the child named on this CIS has:
A verified history of varicella (chickenpox) disease.
Laboratory evidence of immunity (titer) to disease(s) marked below.
Diphtheria |
Hepatitis A |
Hepatitis B |
|
|
|
Hib |
Measles |
Mumps |
|
|
|
Rubella |
Tetanus |
Varicella |
|
|
|
Polio (all 3 serotypes must show immunity)
►
Licensed Health Care Provider Signature Date
►
Printed Name
I certify that the information provided on this form is correct and verifiable.
Health Care Provider or School Official Name: ______________________________ Signature: ______________________ Date:___________
If verified by school or child care staff the medical immunization records must be attached to this document.
Instructions for completing the Certificate of Immunization Status (CIS): Print the from the Immunization Information System (IIS) or fill it in by hand.
To print with the immunization information filled in:
Ask if your health care provider’s office enters immunizations into the WA Immunization Information System (Washington’s statewide registry). If they do, ask them to print the CIS from the IIS and your child’s immunization information will fill in automatically. You can also print a CIS at home by signing up and logging into MyIR at https://wa.myir.net. If your provider doesn’t use the IIS, email or call the Department of Health to get a copy of your child’s CIS: waiisrecords@doh.wa.gov or 1-866-397-0337.
To fill out the form by hand:
1.Print your child’s name and birthdate, and sign your name where indicated on page one.
2.Write the date of each vaccine dose received in the date columns (as MM/DD/YY). If your child receives a combination vaccine (one shot that protects against several diseases), use the Reference Guides below to record each vaccine correctly. For example, record Pediarix under Diphtheria, Tetanus, Pertussis as DTaP, Hepatitis B as Hep B, and Polio as IPV.
3.If your child had chickenpox (varicella) disease and not the vaccine, a health care provider must verify chickenpox disease to meet school requirements.
If your health care provider can verify that your child had chickenpox, ask your provider to check the box in the Documentation of Disease Immunity section and sign the form. If school staff access the IIS and see verification that your child had chickenpox, they will check the box under Varicella in the vaccines section.
4.If your child can show positive immunity by blood test (titer), have your health care provider check the boxes for the appropriate disease in the Documentation of Disease Immunity section, and sign and date the form. You must provide lab reports with this CIS.
5.Provide proof of medically verified records, following the guidelines below.
Acceptable Medical Records
All vaccination records must be medically verified. Examples include:
•A Certificate of Immunization Status (CIS) form printed with the vaccination dates from the Washington State Immunization Information System (IIS), MyIR, or another state’s IIS.
•A completed hardcopy CIS with a health care provider validation signature.
•A completed hardcopy CIS with attached vaccination records printed from a health care provider’s electronic health record with a health care provider signature or stamp. The school administrator, nurse, or designee must verify the dates on the CIS have been accurately transcribed and provide a signature on the form.
Conditional Status
Children can enter and stay in school or child care in conditional status if they are catching up on required vaccines for school or child care entry. (Vaccine series doses are spread out among minimum intervals, so some children may have to wait a period of time before finishing their vaccinations. This means they may enter school while waiting for their next required vaccine dose). To enter school or child care in conditional status, a child must have all the vaccine doses they are eligible to receive before starting school or child care.
Students in conditional status may remain in school while waiting for the minimum valid date of the next vaccine dose plus another 30 days time to turn in documentation of vaccination. If a student is catching up on multiple vaccines, conditional status continues in a similar manner until all of the required vaccines are complete.
If the 30-day conditional period expires and documentation has not been given to the school or child care, then the student must be excluded from further attendance, per RCW 28A.210.120. Valid documentation includes evidence of immunity to the disease in question, medical records showing vaccination, or a completed certificate of exemption (COE) form.
Reference guide for vaccine trade names in alphabetical order |
For updated list, visit https://www.cdc.gov/vaccines/terms/usvaccines.html |
|
|
|
|
|
|
|
|
|
|
|
|
|
Trade Name |
Vaccine |
Trade Name |
Vaccine |
|
Trade Name |
Vaccine |
Trade Name |
Vaccine |
Trade Name |
Vaccine |
|
|
|
|
|
|
|
|
|
|
|
ActHIB |
Hib |
Fluarix |
Flu |
|
Havrix |
Hep A |
Menveo |
Meningococcal |
Rotarix |
Rotavirus (RV1) |
|
|
|
|
|
|
|
|
|
|
|
Adacel |
Tdap |
Flucelvax |
Flu |
|
Hiberix |
Hib |
Pediarix |
DTaP + Hep B + IPV |
RotaTeq |
Rotavirus (PV5) |
|
|
|
|
|
|
|
|
|
|
|
Afluria |
Flu |
FluLaval |
Flu |
|
HibTITER |
Hib |
PedvaxHIB |
Hib |
Tenivac |
Td |
|
|
|
|
|
|
|
|
|
|
|
Bexsero |
MenB |
FluMist |
Flu |
|
Ipol |
IPV |
Pentacel |
DTaP + Hib +IPV |
Trumenba |
MenB |
|
|
|
|
|
|
|
|
|
|
|
Boostrix |
Tdap |
Fluvirin |
Flu |
|
Infanrix |
DTaP |
Pneumovax |
PPSV |
Twinrix |
Hep A + Hep B |
|
|
|
|
|
|
|
|
|
|
|
Cervarix |
2vHPV |
Fluzone |
Flu |
|
Kinrix |
DTaP + IPV |
Prevnar |
PCV |
Vaqta |
Hep A |
|
|
|
|
|
|
|
|
|
|
|
Daptacel |
DTaP |
Gardasil |
4vHPV |
|
Menactra |
MCV or MCV4 |
ProQuad |
MMR + Varicella |
Varivax |
Varicella |
|
|
|
|
|
|
|
|
|
|
|
Engerix-B |
Hep B |
Gardasil 9 |
9vHPV |
|
Menomune |
MPSV4 |
Recombivax HB |
Hep B |
|
|
|
|
|
|
|
|
|
|
|
|
If you have a disability and need this document in another format, please call 1-800-525-0127 (TDD/TTY call 711). |
|
DOH 348-013 June 2021 |