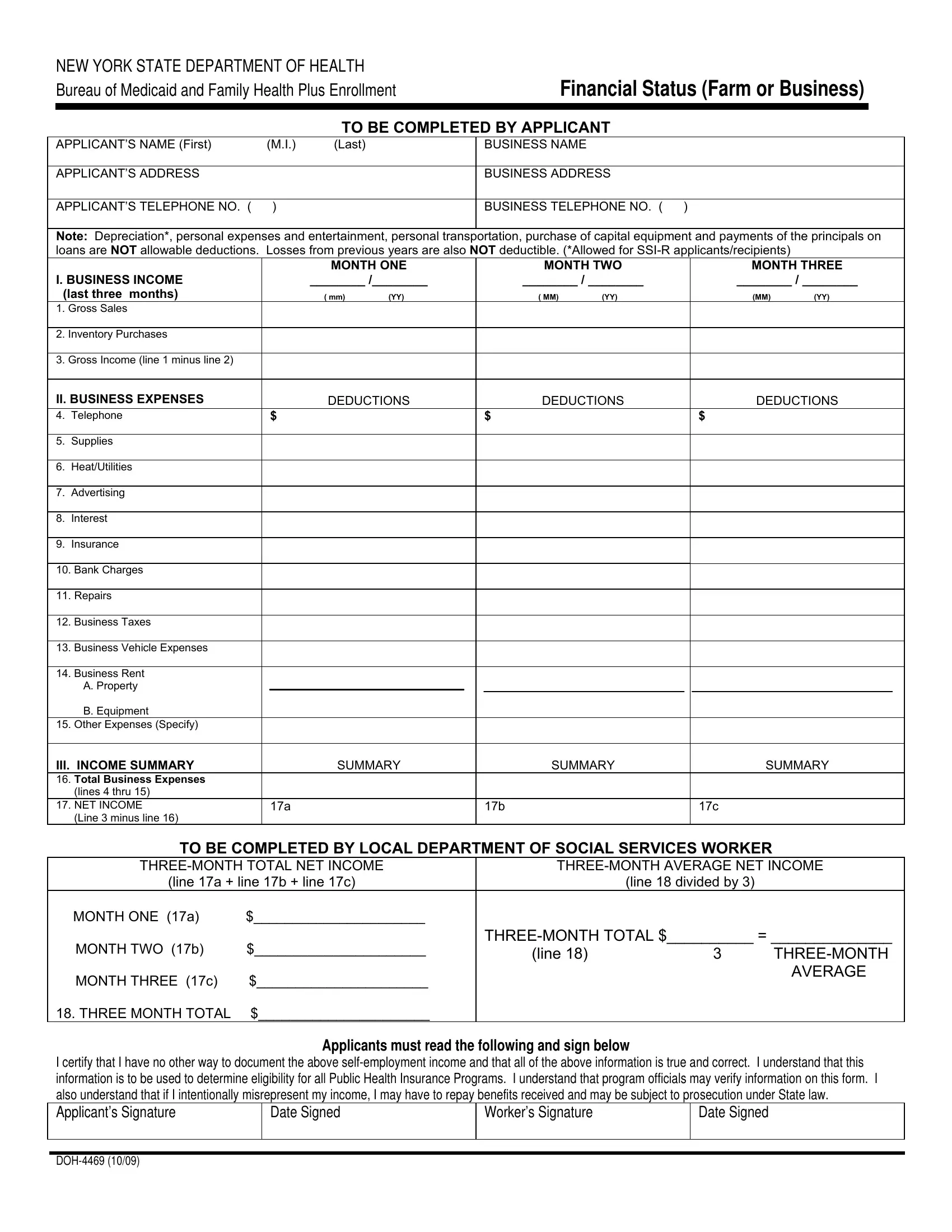
In the intricate world of public health insurance eligibility within New York State, the Department of Health's Doh 4469 form emerges as a critical document for individuals engaged in farming or running a small business. Designed to paint a comprehensive picture of an applicant’s financial status, this form bridges the gap between the self-employed and the often complex eligibility criteria for Medicaid and Family Health Plus programs. Applicants are required to detail both the business and personal aspects of their finances, providing specifics on income, deductions, and expenses over a three-month period. Noteworthy is the stipulation that certain costs—such as depreciation for Social Security Income (SSI-R) applicants/recipients, personal expenses, and entertainment costs—are not considered allowable deductions, thereby excluding them from potentially lowering the reported income. Additionally, the form takes a stringent stance against the deduction of losses from previous years, aiming to ensure a fair and accurate representation of one’s current financial status. The section dedicated to verifying the accuracy and honesty of the provided information underlines the state's commitment to maintaining the integrity of its public health insurance programs. Through the Doh 4469 form, the New York State Department of Health embarks on a meticulous process of determining eligibility, underpinned by the applicant's responsibility to provide a truthful and detailed account of their financial standing.
| Question | Answer |
|---|---|
| Form Name | Doh 4469 Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | month 17c form, doh deductible applicants get, month i 17c pdf, how to doh 4469 |
NEW YORK STATE DEPARTMENT OF HEALTH Bureau of Medicaid and Family Health Plus Enrollment
Financial Status (Farm or Business)
TO BE COMPLETED BY APPLICANT
APPLICANT’S NAME (First) |
(M.I.) |
(Last) |
BUSINESS NAME |
|
|
|
|
APPLICANT’S ADDRESS |
|
|
BUSINESS ADDRESS |
|
|
|
|
APPLICANT’S TELEPHONE NO. ( |
) |
|
BUSINESS TELEPHONE NO. ( ) |
|
|
|
|
Note: Depreciation*, personal expenses and entertainment, personal transportation, purchase of capital equipment and payments of the principals on loans are NOT allowable deductions. Losses from previous years are also NOT deductible. (*Allowed for
|
|
|
|
MONTH ONE |
|
MONTH TWO |
MONTH THREE |
||||||
I. BUSINESS INCOME |
|
________ /________ |
|
________ / ________ |
|
________ / ________ |
|
||||||
(last three months) |
|
|
( mm) |
(YY) |
|
( MM) |
(YY) |
(MM) |
(YY) |
||||
1. |
Gross Sales |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2. |
Inventory Purchases |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
3. |
Gross Income (line 1 minus line 2) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
II. BUSINESS EXPENSES |
|
|
DEDUCTIONS |
|
DEDUCTIONS |
DEDUCTIONS |
|||||||
4. |
Telephone |
|
$ |
|
|
$ |
|
|
$ |
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
5. |
Supplies |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
6. |
Heat/Utilities |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
7. |
Advertising |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
8. |
Interest |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
9. |
Insurance |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
10. Bank Charges |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
11. Repairs |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
12. Business Taxes |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
13. Business Vehicle Expenses |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
14. Business Rent |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
A. Property |
|
|
|
|
|
|
|
|
|
|
|
|
|
B. Equipment |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
15. Other Expenses (Specify) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
III. INCOME SUMMARY |
|
|
SUMMARY |
|
SUMMARY |
SUMMARY |
|||||||
16. Total Business Expenses |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(lines 4 thru 15) |
|
|
|
|
|
|
|
|
|
|
|
|
17. NET INCOME |
|
|
17a |
|
|
|
17b |
|
|
17c |
|
|
|
|
(Line 3 minus line 16) |
|
|
|
|
|
|
|
|
|
|
|
|
|
TO BE COMPLETED BY LOCAL DEPARTMENT OF SOCIAL SERVICES WORKER |
|
|
||||||||||
|
|
|
|
||||||||||
|
(line 17a + line 17b + line 17c) |
|
|
|
|
(line 18 divided by 3) |
|
|
|||||
|
MONTH ONE (17a) |
$______________________ |
|
|
|
|
|
|
|
|
|||
|
MONTH TWO (17b) |
$______________________ |
|
|
|||||||||
|
|
|
(line 18) |
|
|
3 |
|||||||
|
|
|
|
|
|
|
|
|
|
||||
|
MONTH THREE (17c) |
$______________________ |
|
|
|
|
|
|
AVERAGE |
||||
|
|
|
|
|
|
|
|
|
|||||
18. THREE MONTH TOTAL |
$______________________ |
|
|
|
|
|
|
|
|
||||
Applicants must read the following and sign below
I certify that I have no other way to document the above
Applicant’s Signature
Date Signed
Worker’s Signature
Date Signed