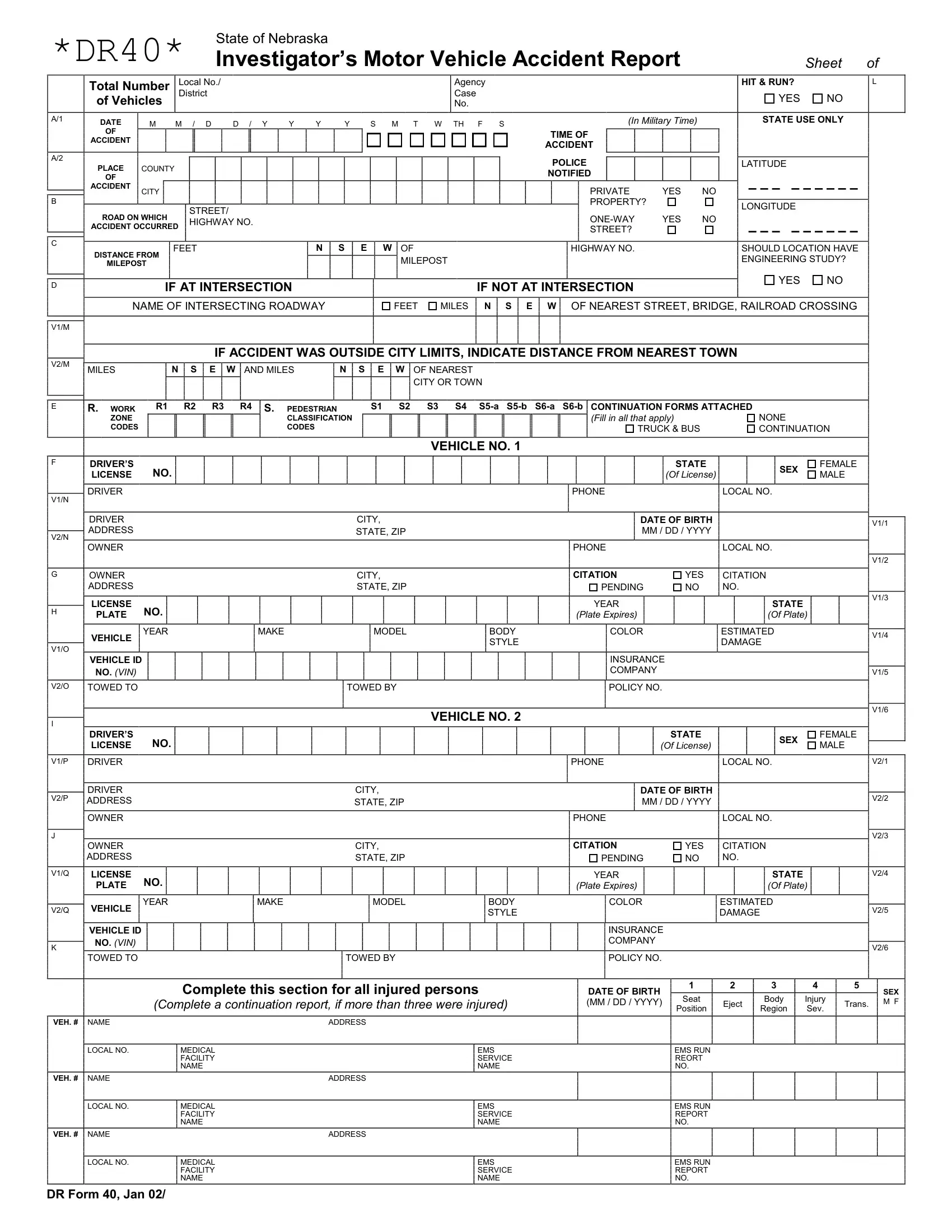
In the State of Nebraska, the DR 40 form is an essential document for law enforcement agencies detailing motor vehicle accidents. Designed to comprehensively record the specifics of the incident, it requires information such as the date, time, and location of the accident, including the county, city, and whether it occurred on a street, road, or highway. The form also probes for details like hit-and-run occurrences, number of vehicles involved, and whether the accident happened on private property or a one-way street. Critical data points such as the latitude and longitude of the accident site are captured to pinpoint the exact location. The form assesses whether the location might need an engineering study, indicating a concern for public safety and infrastructure improvement. Further, it gathers data on whether the accident took place at an intersection, the distance from the nearest town if outside city limits, and details concerning the vehicles and individuals involved, including injuries, vehicle identification numbers (VIN), license information, and insurance details. For accidents with injuries, the form documents the medical facility and EMS service names. This versatile form also includes sections for investigator observations, damaged property, witnesses, vehicle movements before collision, and the extent of damage. Alcohol and drug involvement is scrutinized, showing the form's comprehensive nature in analyzing every aspect of vehicle accidents to improve road safety and accountability.
| Question | Answer |
|---|---|
| Form Name | Dr Form 40 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | nebraska dr 40 fillable form |
*DR40* |
State of Nebraska |
|
Investigator’s Motor Vehicle Accident Report |
Sheet of |
Total Number |
Local No./ |
Agency |
of Vehicles |
District |
Case |
|
No. |
A/1 |
DATE |
M |
M / D |
D / Y |
Y |
Y |
Y |
S M T W TH F S |
||||||||||||
|
||||||||||||||||||||
|
OF |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
ACCIDENT |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
A/2 |
PLACE |
COUNTY |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
OF |
|
|
|
ACCIDENT |
CITY |
|
|
B |
|
||
|
STREET/ |
||
ROAD ON WHICH |
|||
HIGHWAY NO. |
|||
ACCIDENT OCCURRED |
|||
|
|||
|
|
HIT & RUN? |
L |
|
|
YES |
NO |
(In Military Time) |
STATE USE ONLY |
||
TIME OF |
|
|
|
ACCIDENT |
|
|
|
POLICE |
|
LATITUDE |
|
NOTIFIED |
|
|
|
PRIVATE |
YES |
NO |
|
PROPERTY? |
|
LONGITUDE |
|
|
|
|
|
YES |
NO |
|
|
STREET? |
|
|
|
C |
|
FEET |
N S E W OF |
HIGHWAY NO. |
SHOULD LOCATION HAVE |
|
DISTANCE FROM |
||||
|
|
MILEPOST |
|
ENGINEERING STUDY? |
|
|
MILEPOST |
|
|
D |
IF AT INTERSECTION |
IF NOT AT INTERSECTION |
YES |
NO |
|
|
|||
|
|
|
|
|
|
NAME OF INTERSECTING ROADWAY |
FEET MILES N S E W OF NEAREST STREET, BRIDGE, RAILROAD CROSSING |
||
V1/M |
|
|
|
|
IF ACCIDENT WAS OUTSIDE CITY LIMITS, INDICATE DISTANCE FROM NEAREST TOWN
V2/M |
MILES |
N |
S |
E W |
AND MILES |
N S |
E |
W |
OF NEAREST |
|
|||||||||
|
|
|
|
|
|
|
|
|
CITY OR TOWN |
E |
R. WORK |
R1 |
R2 |
R3 |
R4 S. PEDESTRIAN |
|
S1 |
S2 |
S3 S4 |
|
ZONE |
|
|
|
CLASSIFICATION |
|
|
(Fill in all that apply) |
|
|
CODES |
|
|
|
CODES |
|
|
|
TRUCK & BUS |
NONE CONTINUATION
VEHICLE NO. 1
F |
DRIVER’S |
NO. |
|
LICENSE |
|
V1/N |
DRIVER |
|
|
|
|
|
DRIVER |
CITY, |
V2/N |
ADDRESS |
STATE, ZIP |
OWNER |
|
|
|
|
|
G |
OWNER |
CITY, |
|
ADDRESS |
STATE, ZIP |
H |
LICENSE |
NO. |
|
|
|
PLATE |
|
|
|
||
|
VEHICLE |
YEAR |
MAKE |
MODEL |
BODY |
V1/O |
|
|
|
STYLE |
|
|
|
|
|
||
VEHICLE ID |
|
|
|
|
|
|
|
|
|
|
|
|
NO. (VIN) |
|
|
|
|
V2/O |
TOWED TO |
|
|
TOWED BY |
|
I |
|
|
|
|
VEHICLE NO. 2 |
DRIVER’S |
|
|
|
|
|
|
NO. |
|
|
|
|
|
LICENSE |
|
|
|
|
V1/P |
DRIVER |
|
|
|
|
V2/P |
DRIVER |
|
|
CITY, |
|
ADDRESS |
|
|
STATE, ZIP |
|
|
|
OWNER |
|
|
|
|
J |
OWNER |
|
|
CITY, |
|
|
|
|
|
||
|
ADDRESS |
|
|
STATE, ZIP |
|
V1/Q |
LICENSE |
NO. |
|
|
|
|
PLATE |
|
|
|
|
V2/Q |
VEHICLE |
YEAR |
MAKE |
MODEL |
BODY |
|
|
|
STYLE |
||
|
|
|
|
|
|
|
VEHICLE ID |
|
|
|
|
K |
NO. (VIN) |
|
|
|
|
TOWED TO |
|
|
TOWED BY |
|
|
|
|
|
|
Complete this section for all injured persons
(Complete a continuation report, if more than three were injured)
VEH. # |
NAME |
|
ADDRESS |
|
LOCAL NO. |
MEDICAL |
EMS |
|
|
FACILITY |
SERVICE |
|
|
NAME |
NAME |
VEH. # |
NAME |
|
ADDRESS |
|
LOCAL NO. |
MEDICAL |
EMS |
|
|
FACILITY |
SERVICE |
|
|
NAME |
NAME |
VEH. # |
NAME |
|
ADDRESS |
|
LOCAL NO. |
MEDICAL |
EMS |
|
|
FACILITY |
SERVICE |
|
|
NAME |
NAME |
|
STATE |
|
SEX |
FEMALE |
|
|
|
(Of License) |
|
MALE |
|
||
|
|
|
|
|||
PHONE |
|
LOCAL NO. |
|
|
|
|
DATE OF BIRTH |
|
|
|
|
V1/1 |
|
MM / DD / YYYY |
|
|
|
|
|
|
PHONE |
|
LOCAL NO. |
|
|
|
|
|
|
|
|
|
|
V1/2 |
CITATION |
YES |
CITATION |
|
|
|
|
PENDING |
NO |
NO. |
|
|
|
V1/3 |
YEAR |
|
|
STATE |
|
|
|
|
|
|
|
|
||
(Plate Expires) |
|
|
(Of Plate) |
|
|
|
COLOR |
|
ESTIMATED |
|
|
V1/4 |
|
|
|
DAMAGE |
|
|
||
|
|
|
|
|
||
INSURANCE |
|
|
|
|
|
|
COMPANY |
|
|
|
|
|
V1/5 |
POLICY NO. |
|
|
|
|
|
|
|
|
|
|
|
|
V1/6 |
|
STATE |
|
SEX |
FEMALE |
|
|
(Of License) |
|
MALE |
|
|||
|
|
|
||||
PHONE |
|
LOCAL NO. |
|
|
V2/1 |
|
DATE OF BIRTH |
|
|
|
|
V2/2 |
|
MM / DD / YYYY |
|
|
|
|
||
PHONE |
|
LOCAL NO. |
|
|
|
|
CITATION |
YES |
CITATION |
|
|
V2/3 |
|
|
|
|
||||
PENDING |
NO |
NO. |
|
|
|
|
YEAR |
|
|
STATE |
|
|
V2/4 |
(Plate Expires) |
|
|
(Of Plate) |
|
|
|
COLOR |
|
ESTIMATED |
|
|
V2/5 |
|
|
|
DAMAGE |
|
|
|
|
INSURANCE |
|
|
|
|
|
|
COMPANY |
|
|
|
|
|
V2/6 |
POLICY NO. |
|
|
|
|
|
|
|
|
|
|
|
|
|
DATE OF BIRTH |
1 |
2 |
3 |
4 |
5 |
SEX |
Seat |
|
Body |
Injury |
|
||
(MM / DD / YYYY) |
Eject |
Trans. M F |
||||
|
Position |
|
Region |
Sev. |
|
|
EMS RUN
REORT
NO.
EMS RUN
REPORT
NO.
EMS RUN
REPORT
NO.
DR Form 40, Jan 02/
THE FOLLOWING INFORMATION IS REQUIRED FOR ALL ACCIDENTS
|
Investigation |
INDICATE BY DIAGRAM WHAT HAPPENED |
Agency Case No.: |
|
|
made at scene? |
|
||
Indicate North |
Yes |
No |
|
|
by Arrow |
|
|
||
|
|
|
|
|
DESCRIPTION OF ACCIDENT BASED ON OFFICER’S INVESTIGATION
PROPERTY
OBJECT DAMAGED
OBJECT DAMAGED
OWNER NAME |
ADDRESS |
PHONE |
APPROX. COST OF DAMAGE |
OWNER NAME |
ADDRESS |
PHONE |
APPROX. COST OF DAMAGE |
WITNESSES |
|
NAME |
|
|
|
|
ADDRESS |
|
|
|
|
PHONE |
|
|
||
|
NAME |
|
|
|
|
ADDRESS |
|
|
|
|
PHONE |
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
VEHICLE MOVEMENT |
POINT OF IMPACT AND |
|
AIRBAG DEPLOYED |
|
RESTRAINT USE |
TOTAL |
VEH |
VEH |
|||||
|
|
|
BEFORE COLLISION |
MOST DAMAGED AREA |
|
|
||||||||||
|
|
|
|
|
OCCUPANTS |
1 |
2 |
|
||||||||
VEH. |
|
|
ROAD OR |
(Enter numbers for each vehicle) |
|
|
|
|
|
|||||||
N S E W |
|
|
|
|
|
|
|
|
|
|
||||||
NO. |
|
HIGHWAY NAME |
VEHICLE 1 |
VEHICLE 2 |
|
VEHICLE 1 |
|
VEHICLE 1 |
ALCOHOL |
Driver |
Driver |
Pedes- |
||||
1 |
|
|
|
|
|
POINT |
POINT |
|
|
|
|
TESTING |
No. 1 |
No. 2 |
trian |
|
|
|
|
|
|
OF |
OF |
|
|
|
|
ALCOHOL |
Y |
Y |
Y |
||
2 |
|
|
|
|
|
IMPACT |
IMPACT |
|
|
|
|
|||||
|
|
|
|
|
MOST |
MOST |
|
|
|
|
LEVEL |
N |
N |
N |
||
|
|
|
|
|
DAMAGED |
DAMAGED |
1 Deployed – front |
1 |
None used – vehicle occupant |
|||||||
|
|
|
|
|
|
AREA |
AREA |
TESTED |
||||||||
1 |
|
|
|
07 |
Making |
|
|
2 Deployed – side |
2 |
Lap & shoulder belt used |
BAC LEVEL |
|
|
|
||
|
|
|
|
|
3 |
Shoulder belt only used |
|
|
|
|||||||
|
|
|
|
|
|
3 |
Deployed – both front/side |
|
|
|
||||||
|
|
|
|
08 |
Entering |
|
|
4 |
Not deployed |
4 |
Lap belt only used |
ALCOHOL/ |
Driver |
|
Driver |
|
2 |
|
|
|
|
|
5 |
Child safety seat used |
|
||||||||
|
|
|
|
traffic lane |
|
|
5 |
Not applicable/No airbag available |
6 |
Child booster seat used |
DRUGS |
No. 1 |
|
No. 2 |
||
|
|
|
|
09 |
Leaving |
|
|
6 Unknown |
7 |
Helmet used |
SUSPECTED |
|
|
|
||
01 |
Essentially straight |
|
traffic lane |
|
|
|
|
8 |
Restraint use unknown |
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|||||||
02 |
ahead |
10 |
Parked |
|
|
|
VEHICLE 2 |
|
VEHICLE 2 |
1 |
Neither alcohol nor drugs suspected |
|||||
Backing |
11 |
Slowing or |
|
|
|
|
|
|
2 |
Yes – alcohol suspected |
|
|||||
03 |
Changing lanes |
|
stopped in |
|
|
|
|
|
|
|
||||||
04 |
Overtaking/ |
|
traffic |
00 None |
11 Total (all areas) |
|
|
|
|
3 Yes – drugs suspected |
|
|
||||
|
Passing |
12 |
Other |
|
|
|
|
4 |
Yes – alcohol & drugs suspected |
|
||||||
05 |
Turning right |
09 Top & windows |
12 Other |
|
|
|
|
|
||||||||
13 |
Unknown |
|
|
|
|
5 Unknown |
|
|
|
|||||||
06 |
Turning left |
10 Undercarriage |
|
|
|
|
|
|
|
|
||||||
OFFICER NO. |
|
TROOP/ |
DEPARTMENT |
|
|
|
|
Photographs |
YES |
|||||||
|
|
|
|
|
TEAM/ |
|
|
|
|
|
|
|
||||
|
|
|
|
|
BEAT |
|
|
|
|
|
|
|
taken? |
NO |
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
INVESTIGATOR NAME (Print or Type) |
|
|
INVESTIGATOR SIGNATURE |
|
|
|
DATE OF |
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
REPORT