

Using the online PDF tool by FormsPal, you are able to fill in or modify aca form 1843 right here and now. To retain our editor on the leading edge of practicality, we aim to put into operation user-oriented capabilities and improvements on a regular basis. We are at all times looking for suggestions - play a vital role in reshaping how we work with PDF documents. To get the process started, take these basic steps:
Step 1: Hit the "Get Form" button above. It'll open our editor so that you could start filling out your form.
Step 2: When you open the PDF editor, you will find the document all set to be filled out. In addition to filling in different blank fields, you could also do several other things with the form, including adding any text, modifying the initial text, inserting graphics, putting your signature on the PDF, and more.
As for the fields of this precise PDF, here is what you should know:
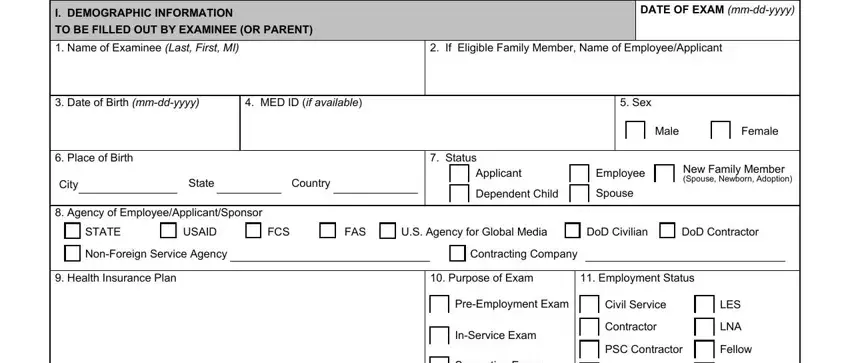
1. The aca form 1843 involves specific details to be inserted. Make certain the next blanks are completed:
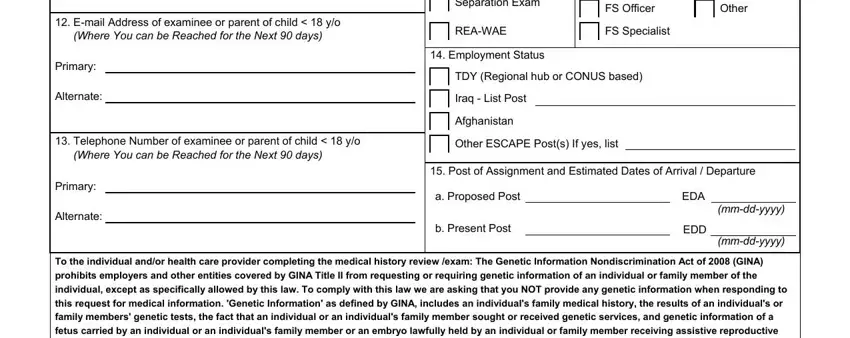
2. The subsequent part is to submit the next few blank fields: Separation Exam, FS Officer, Other, Email Address of examinee or, Primary, Alternate, REAWAE, FS Specialist, Employment Status, TDY Regional hub or CONUS based, Iraq List Post, Afghanistan, Telephone Number of examinee or, Other ESCAPE Posts If yes list, and Primary.
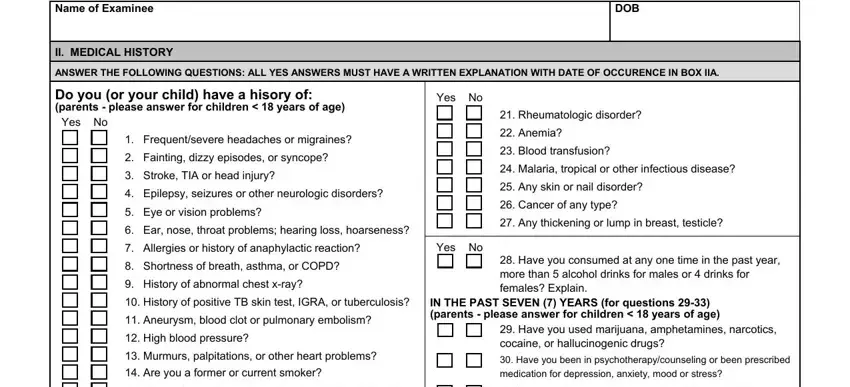
3. Completing Name of Examinee, II MEDICAL HISTORY, DOB, ANSWER THE FOLLOWING QUESTIONS ALL, Do you or your child have a hisory, Yes, Yes, Frequentsevere headaches or, Fainting dizzy episodes or syncope, Stroke TIA or head injury, Epilepsy seizures or other, Eye or vision problems, Ear nose throat problems hearing, Allergies or history of, and Yes No is essential for the next step, make sure to fill them out in their entirety. Don't miss any details!
4. To move ahead, the next form section involves filling out a handful of fields. Examples include Stomach esophageal or other, Have you felt unusually depressed, Jaundice hepatitis or other liver, Intestinal rectal problems or, Urinary or kidney problems blood, Diabetes thyroid or other, Joint or back paininjury, crying spells which lasted more, Have you had frequent or, Have you experienced any, Children Only Has your child been, Yes, Women provide results if, Colon Cancer Screening Submit, and Date of last PAP test Results, which you'll find crucial to moving forward with this process.
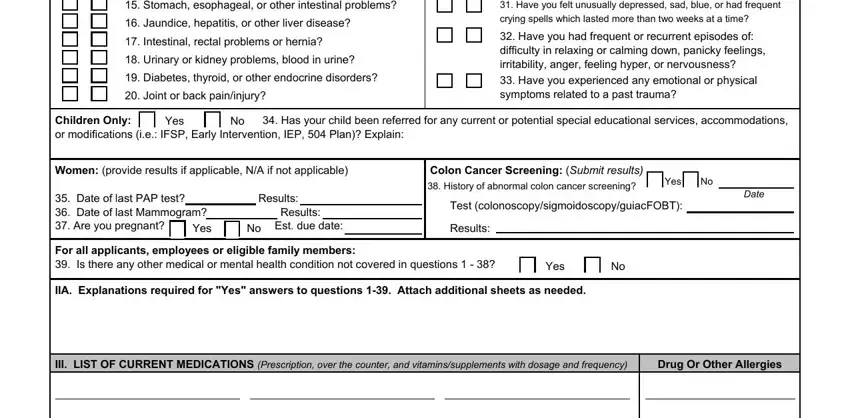
It's simple to make an error when completing the Diabetes thyroid or other, so you'll want to reread it prior to deciding to submit it.
5. While you reach the end of the file, you'll notice a couple extra things to undertake. In particular, Date mmddyyyy, Illness or Operation, Name of Hospital, City and State, Any knowing and willful omission, V SIGNATURE OF EXAMINEE OR PARENT, Date mmddyyyy, and Page of must be filled in.
Step 3: Check that the details are correct and press "Done" to conclude the task. Try a 7-day free trial account with us and gain direct access to aca form 1843 - download, email, or edit in your personal account page. FormsPal ensures your data privacy by using a protected method that never records or shares any kind of private data used. Be assured knowing your docs are kept confidential when you use our tools!