
When using the online editor for PDFs by FormsPal, you are able to fill out or alter ds police ny right here and now. FormsPal team is devoted to providing you the perfect experience with our tool by consistently presenting new capabilities and upgrades. With these updates, working with our tool gets better than ever before! With a few easy steps, you can begin your PDF journey:
Step 1: Hit the orange "Get Form" button above. It will open up our pdf tool so that you could begin completing your form.
Step 2: This tool helps you modify your PDF form in a variety of ways. Modify it by adding your own text, correct original content, and add a signature - all within the reach of a couple of mouse clicks!
This PDF doc requires specific information; in order to guarantee accuracy and reliability, take the time to take note of the guidelines just below:
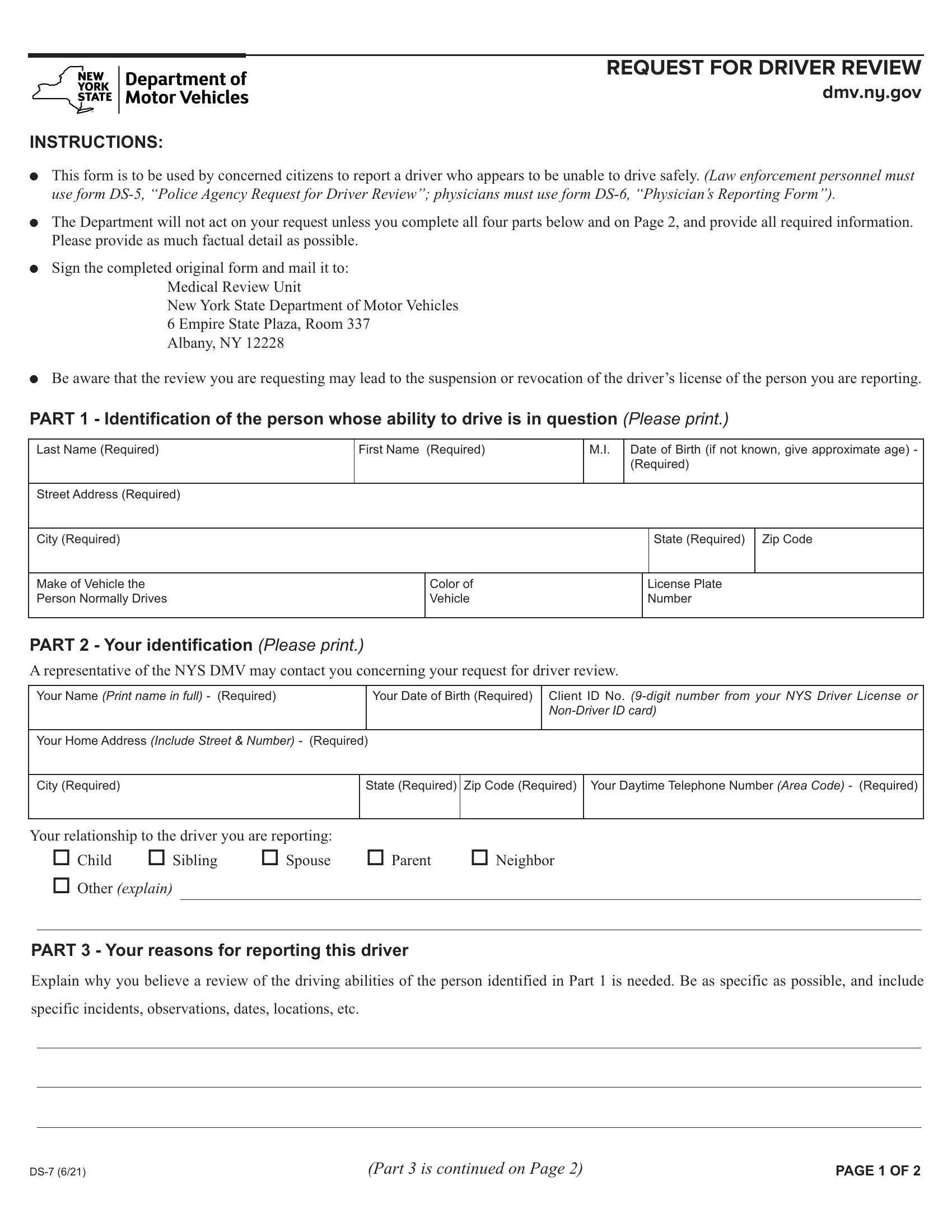
1. The ds police ny necessitates specific information to be typed in. Ensure the subsequent blank fields are complete:
2. Once your current task is complete, take the next step – fill out all of these fields - Your relationship to the driver, Other explain, PART Your reasons for reporting, Explain why you believe a review, specific incidents observations, Part is continued on Page, and PAGE OF with their corresponding information. Make sure to double check that everything has been entered correctly before continuing!
3. In this step, look at PART Continued from Page, and If you know other people who agree. All of these must be filled out with highest precision.
In terms of PART Continued from Page and If you know other people who agree, ensure that you get them right in this section. The two of these could be the most significant fields in the form.
4. The following part comes next with the following blanks to fill out: Name, Name, Name, Name, Address, Address, Address, Address, Daytime Telephone Number, Daytime Telephone Number, Daytime Telephone Number, Daytime Telephone Number, PART CERTIFICATION I certify, Your Signature Sign name in full, and Date MonthDayYear.
Step 3: Ensure that the information is correct and press "Done" to conclude the project. Get your ds police ny the instant you register here for a 7-day free trial. Readily access the pdf file in your FormsPal account, along with any edits and adjustments being automatically synced! We do not sell or share any details you use when filling out documents at FormsPal.