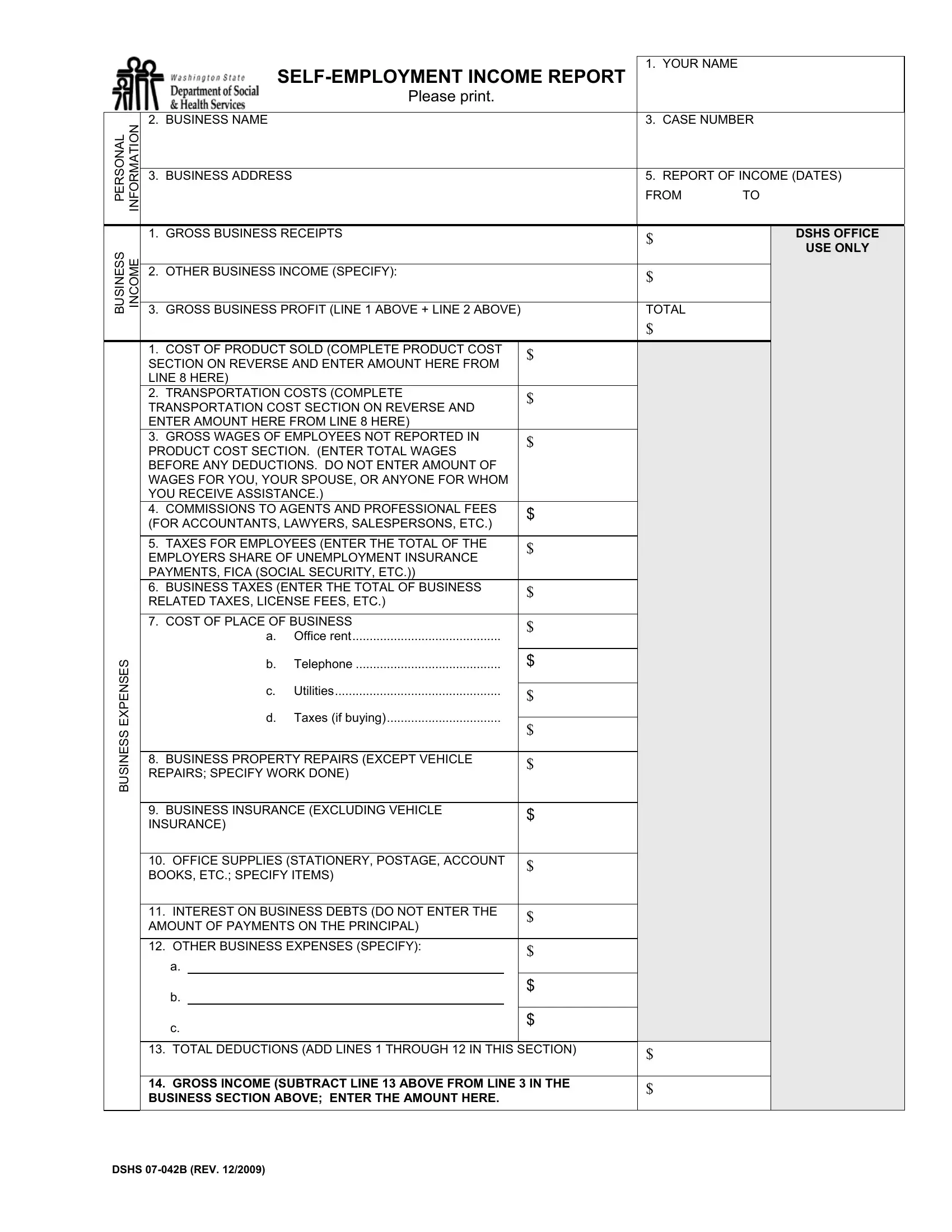
For individuals navigating the complexities of reporting self-employed income, the Department of Social and Health Services (DSHS) Self-Employment Income Report form provides a structured means to present their financial activities accurately. This detailed form not only requests personal information, such as the individual's name and business address, but also delves deeply into the specifics of business income and expenses. It facilitates a thorough breakdown of earnings by asking for gross business receipts, other business income, and the calculation of gross business profit. Moreover, it comprehensively addresses the expense side of business operations, covering everything from the cost of product sold, transportation costs, wages of employees (excluding the business owner, spouse, or dependents), and a suite of other operational expenses including office rent, utility costs, and business insurance. The form also includes sections for reporting the cost associated with the production of goods, including the cost of materials and direct salaries related to product manufacturing. Importantly, it provides options for calculating transportation costs, allowing for the deduction of vehicle-related expenses, thereby acknowledging the diverse nature of business expenditures. The added layer of verification and the requirement for signatures under the penalty of perjury underscore the form's role in ensuring accurate and honest reporting. By offering a detailed framework for self-employed individuals to report their income and expenses, the DSHS Self-Employment Income Report form plays a crucial role in facilitating accurate social and health service support assessments.
| Question | Answer |
|---|---|
| Form Name | Dshs Self Employment Form |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | dshs self report, dshs self employment, dshs self, 07 042b |
Please print.
1. YOUR NAME
PERSONAL |
INFORMATION |
2. |
BUSINESS NAME |
3. |
CASE NUMBER |
|
|
|
|
|
|
3. |
BUSINESS ADDRESS |
5. |
REPORT OF INCOME (DATES) |
|
|
|
FROM |
TO |
|
|
|
|
|
|
BUSINESS |
INCOME |
BUSINESS EXPENSES
1. GROSS BUSINESS RECEIPTS |
|
$ |
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2. OTHER BUSINESS INCOME (SPECIFY): |
|
$ |
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
3. GROSS BUSINESS PROFIT (LINE 1 ABOVE + LINE 2 ABOVE) |
|
TOTAL |
|||||
|
|
|
|
|
|
$ |
|
1. COST OF PRODUCT SOLD (COMPLETE PRODUCT COST |
|
$ |
|
|
|||
|
|
|
|||||
SECTION ON REVERSE AND ENTER AMOUNT HERE FROM |
|
|
|
||||
|
|
|
|
||||
LINE 8 HERE) |
|
|
|
|
|
|
|
2. TRANSPORTATION COSTS (COMPLETE |
|
$ |
|
|
|||
TRANSPORTATION COST SECTION ON REVERSE AND |
|
|
|
||||
|
|
|
|
||||
ENTER AMOUNT HERE FROM LINE 8 HERE) |
|
|
|
|
|||
3. GROSS WAGES OF EMPLOYEES NOT REPORTED IN |
|
$ |
|
|
|||
PRODUCT COST SECTION. (ENTER TOTAL WAGES |
|
|
|
||||
|
|
|
|
||||
BEFORE ANY DEDUCTIONS. DO NOT ENTER AMOUNT OF |
|
|
|
|
|||
WAGES FOR YOU, YOUR SPOUSE, OR ANYONE FOR WHOM |
|
|
|
|
|||
YOU RECEIVE ASSISTANCE.) |
|
|
|
|
|||
4. COMMISSIONS TO AGENTS AND PROFESSIONAL FEES |
|
$ |
|
|
|||
(FOR ACCOUNTANTS, LAWYERS, SALESPERSONS, ETC.) |
|
|
|
||||
|
|
|
|
||||
|
|
|
|
|
|
|
|
5. TAXES FOR EMPLOYEES (ENTER THE TOTAL OF THE |
|
$ |
|
|
|||
EMPLOYERS SHARE OF UNEMPLOYMENT INSURANCE |
|
|
|
||||
|
|
|
|
||||
PAYMENTS, FICA (SOCIAL SECURITY, ETC.)) |
|
|
|
|
|||
6. BUSINESS TAXES (ENTER THE TOTAL OF BUSINESS |
|
$ |
|
|
|||
RELATED TAXES, LICENSE FEES, ETC.) |
|
|
|
||||
|
|
|
|
||||
|
|
|
|
|
|
|
|
7. COST OF PLACE OF BUSINESS |
|
$ |
|
|
|||
|
a. |
Office rent |
|
|
|
||
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
b. |
Telephone |
|
$ |
|
|
|
|
c. |
Utilities |
|
|
|
|
|
|
|
$ |
|
|
|||
|
|
|
|
|
|
|
|
|
d. |
Taxes (if buying) |
|
|
|
|
|
|
$ |
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
8. BUSINESS PROPERTY REPAIRS (EXCEPT VEHICLE |
|
$ |
|
|
|||
REPAIRS; SPECIFY WORK DONE) |
|
|
|
||||
|
|
|
|
||||
|
|
|
|
|
|
|
|
9. BUSINESS INSURANCE (EXCLUDING VEHICLE |
|
$ |
|
|
|||
INSURANCE) |
|
|
|
|
|
||
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
10. OFFICE SUPPLIES (STATIONERY, POSTAGE, ACCOUNT |
|
$ |
|
|
|||
BOOKS, ETC.; SPECIFY ITEMS) |
|
|
|
|
|||
|
|
|
|
|
|
|
|
11. INTEREST ON BUSINESS DEBTS (DO NOT ENTER THE |
|
$ |
|
|
|||
AMOUNT OF PAYMENTS ON THE PRINCIPAL) |
|
|
|
||||
|
|
|
|
||||
|
|
|
|
|
|||
12. OTHER BUSINESS EXPENSES (SPECIFY): |
|
$ |
|
|
|||
|
|
|
|
|
|
|
|
a. |
|
|
|
|
|
|
|
b. |
|
|
|
$ |
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
c. |
|
|
|
$ |
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
||
13. TOTAL DEDUCTIONS (ADD LINES 1 THROUGH 12 IN THIS SECTION) |
$ |
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|||||
14. GROSS INCOME (SUBTRACT LINE 13 ABOVE FROM LINE 3 IN THE |
$ |
|
|||||
BUSINESS SECTION ABOVE; ENTER THE AMOUNT HERE. |
|
|
|||||
|
|
|
|||||
|
|
|
|
|
|
|
|
DSHS OFFICE
USE ONLY
DSHS
|
1. |
INVENTORY AT BEGINNING OF MONTH (IF DIFFERENT THAN END OF LAST |
|
|
MONTH'S, ATTACH EXPLANATION - ENTER DOLLAR VALUE) |
||
|
2. |
COST OF MATERIALS USED TO MAKE PRODUCT (SPECIFY MATERIALS) |
|
|
3. |
COST OF PRODUCT IF YOU DO NOT MAKE PRODUCT |
|
|
4. |
SALARIES (BEFORE DEDUCTIONS) OF EMPLOYEES WHO MAKE PRODUCT. |
|
COST |
DO NOT INCLUDE WAGES OF ANYONE FOR WHOM YOU RECEIVE |
||
ASSISTANCE. |
|||
5. OTHER PRODUCT RELATED COSTS (SPECIFY BELOW) |
|||
PRODUCT |
|
a. |
|
|
|
||
|
|
b. |
|
|
|
c. |
|
|
6. |
TOTAL PRODUCT COST (ADD LINES 1 THROUGH 5 ABOVE) |
|
|
7. |
INVENTORY AT END OF MONTH (ENTER DOLLAR VALUE) |
|
|
8. |
PRODUCT COST (SUBTRACT LINE 7 ABOVE FROM LINE 6 ABOVE. ENTER |
|
|
HERE AND ON THE REVERSE SIDE OF THIS FORM IN THE BUSINESS |
||
|
EXPENSES SECTION, LINE 1) |
||
|
1. |
ENTER TOTAL MILES DRIVEN ON THE JOB |
|
2.ENTER TOTAL MILES DRIVEN THIS MONTH (ON AND OFF THE JOB)
3.PERCENTAGE OF MILES DRIVEN FOR BUSINESS PURPOSES (DIVIDE MILES IN LINE 1 ABOVE BY MILES IN LINE 2 ABOVE. ANSWER SHOULD BE A DECIMAL.)
COST |
4. VEHICLE SERVICING OR REPAIRS PAID THIS MONTH |
$ |
|
|
|
||
|
|
|
|
5. REGISTRATION AND LICENSE FEES PAID THIS MONTH |
$ |
||
TRANSPORTATION |
|
|
|
|
|
|
|
ONECHECK |
|
|
|
|
6. INTEREST ON VEHICLE PAYMENTS PAID THIS MONTH |
$ |
|
|
|
I want to deduct $.55 per mile for gas, oil and fluids. |
$ |
|
|
MULTIPLY NUMBER OF MILES IN LINE 2 BY $.485. |
|
|
|
ENTER AMOUNT. |
|
|
|
I want to itemize the following expenses: Gasoline |
$ |
|
|
|
|
|
|
|
|
|
|
Oil |
$ |
|
|
Fluids |
|
|
|
$ |
|
|
|
|
|
|
|
|
|
7.TOTAL TRANSPORTATION COSTS THIS MONTH. ADD LINES 4 THROUGH 6 ABOVE AND ENTER AMOUNT.
8.MULTIPLY AMOUNT IN LINE 7 ABOVE BY THE NUMBER IN LINE 3 ABOVE. ENTER HERE AND ON THE REVERSE SIDE OF THIS FORM IN THE BUSINESS EXPENSES SECTION, LINE 2)
CHECK AND COMPLETE IF STATEMENT APPLIES TO YOU DATE OF LAST DAY WORKED
|
$ |
|
|
DSHS OFFICE |
|
|
|
USE ONLY |
|
|
|
|
|
|
|
$ |
|
|
|
|
$ |
|
|
|
|
|
|
|
|
|
$ |
|
|
|
|
$ |
|
|
|
|
$ |
|
|
|
|
$ |
|
|
|
|
$ |
|
|
|
|
$ |
|
|
|
|
$ |
|
|
|
|
|
|
|
|
|
|
|
|
|
$
$
DATE INCOME DUE |
AMOUNT |
I am no longer |
|
|
$ |
|
|
|
|
READ CAREFULLY AND SIGN BEFORE RETURNING YOUR REPORT
1.I understand that I must verify all income and deductions claimed. I hereby authorize the department to contact other persons or agencies to obtain necessary information regarding my income.
2.I understand that information given in this report may result in the reduction, suspension or termination of my grant.
3.I declare under penalty of perjury that information given in this report is true and correct to the best of my knowledge. (Both husband and wife must sign if living together.)
YOUR SIGNATURE |
DATE |
YOUR SPOUSE’S SIGNATURE |
DATE |
DSHS