
When using the online tool for PDF editing by FormsPal, you can easily complete or change 8113 form right here. To maintain our editor on the forefront of practicality, we aim to integrate user-driven features and enhancements on a regular basis. We're at all times looking for feedback - join us in reshaping PDF editing. It merely requires a couple of simple steps:
Step 1: Just click on the "Get Form Button" above on this site to start up our pdf file editor. This way, you will find all that is necessary to work with your file.
Step 2: With this advanced PDF file editor, you can accomplish more than just complete blank form fields. Try all the functions and make your documents seem professional with customized textual content added in, or fine-tune the original content to excellence - all accompanied by an ability to add any type of images and sign the PDF off.
It's straightforward to fill out the form adhering to this practical guide! This is what you want to do:
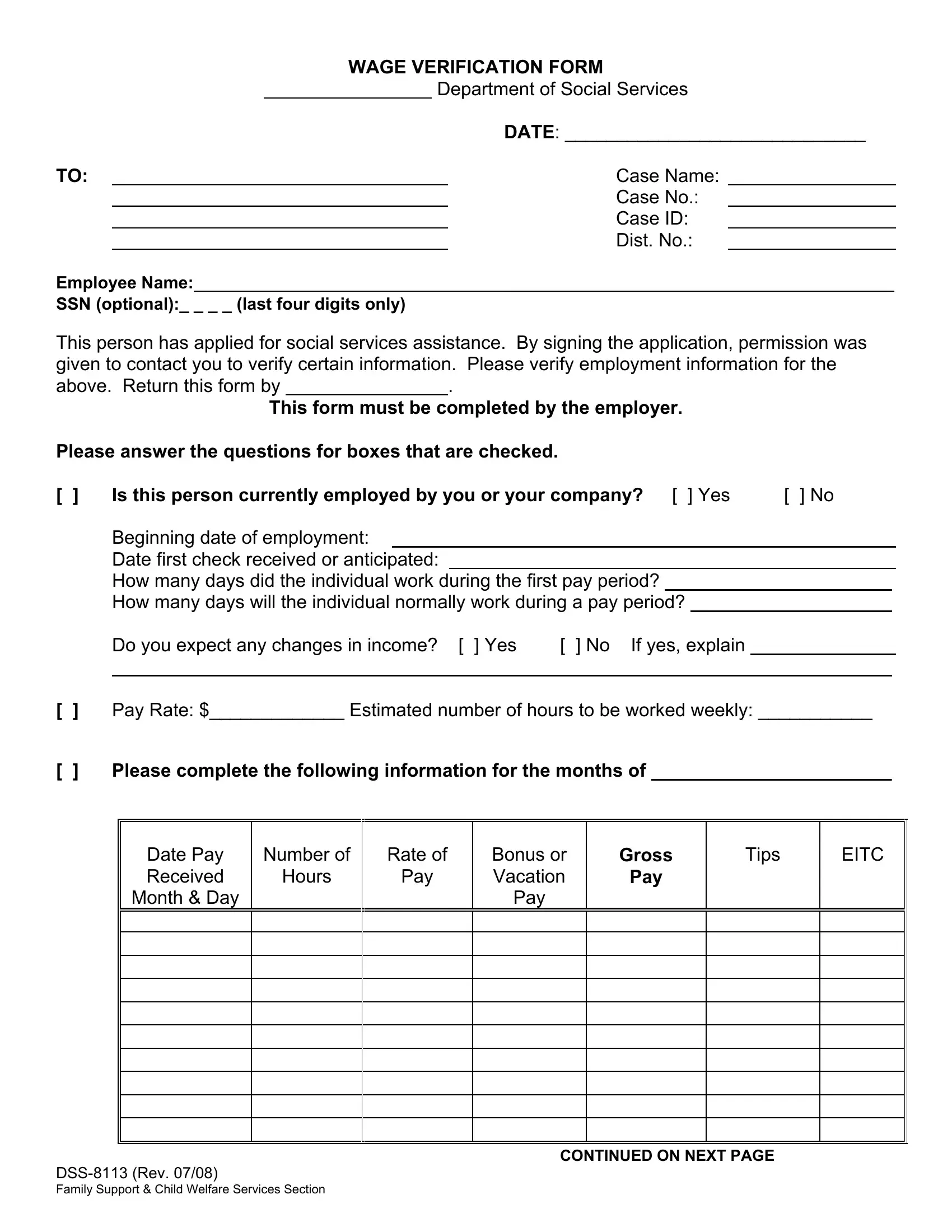
1. The 8113 form necessitates certain information to be typed in. Ensure that the following blank fields are filled out:
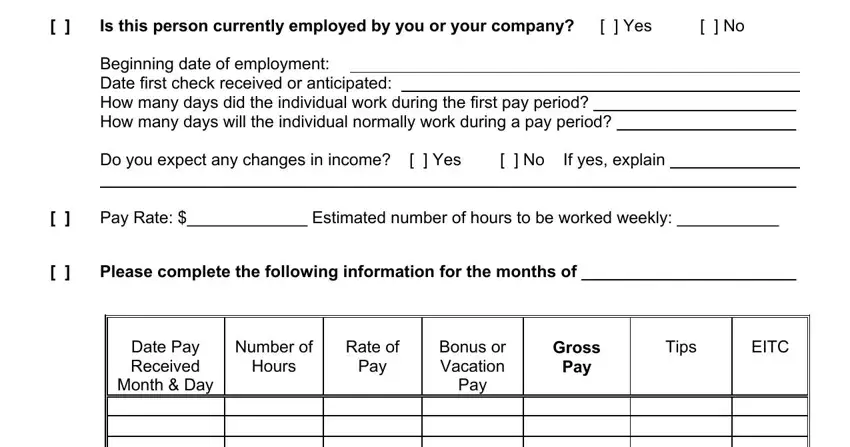
2. Right after finishing the last step, head on to the subsequent part and enter the essential details in all these blank fields - Is this person currently employed, Please answer the questions for, Beginning date of employment Date, Do you expect any changes in, No If yes explain, Yes, Pay Rate Estimated number of, Please complete the following, Date Pay Received, Number of, Rate of, Hours, Pay, Month Day, and Bonus or Vacation.
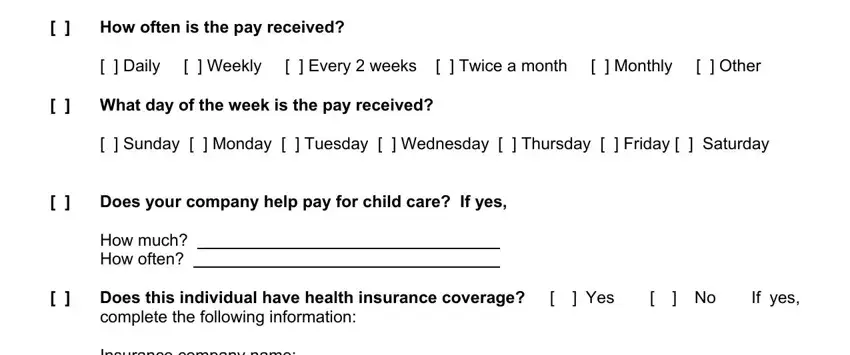
3. Completing How often is the pay received, What day of the week is the, How much How often, Does your company help pay for, Daily Weekly Every weeks, Sunday Monday Tuesday, Does this individual have health, Yes No If yes, Insurance company name Certificate, and Effective date of coverage is essential for the next step, make sure to fill them out in their entirety. Don't miss any details!
It's easy to make a mistake when filling in the Insurance company name Certificate, so make sure to take another look prior to when you submit it.
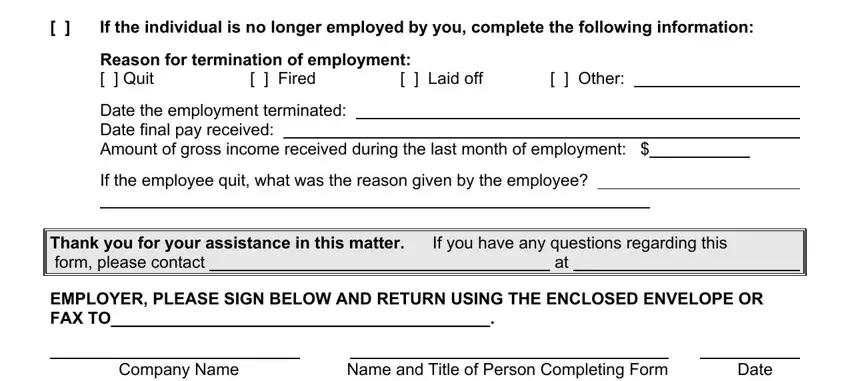
4. To go ahead, this fourth step will require filling in a few blanks. Included in these are If the individual is no longer, Reason for termination of, Fired, Laid off, Other, Date the employment terminated, If the employee quit what was the, Company Name, Thank you for your assistance in, Name and Title of Person, and Date, which are fundamental to carrying on with this particular PDF.
Step 3: Look through what you have typed into the blank fields and click the "Done" button. Right after getting afree trial account here, it will be possible to download 8113 form or email it at once. The PDF will also be readily available via your personal account page with your edits. FormsPal offers secure document completion devoid of personal data recording or sharing. Be assured that your information is in good hands here!