
You may fill in Dss Form 1606 instantly using our PDFinity® editor. Our development team is continuously endeavoring to enhance the tool and insure that it is much easier for people with its extensive features. Discover an ceaselessly innovative experience today - take a look at and uncover new opportunities as you go! Here's what you'll have to do to begin:
Step 1: Just hit the "Get Form Button" in the top section of this site to open our pdf file editor. Here you'll find all that is needed to work with your file.
Step 2: With the help of this advanced PDF file editor, it's possible to accomplish more than just fill out blanks. Express yourself and make your docs appear professional with customized textual content added, or tweak the file's original input to perfection - all accompanied by the capability to incorporate any kind of pictures and sign it off.
It is actually straightforward to complete the form with this detailed guide! Here's what you should do:
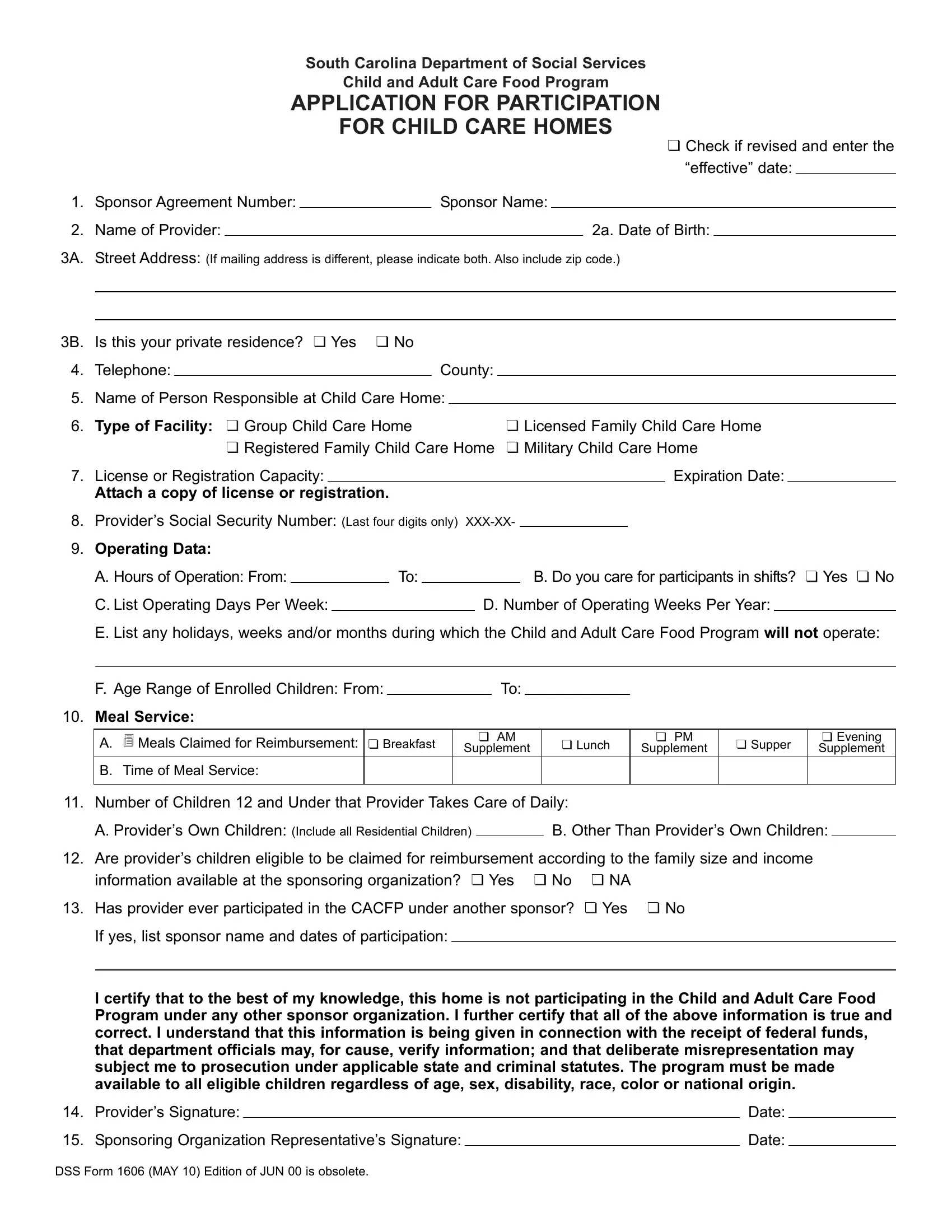
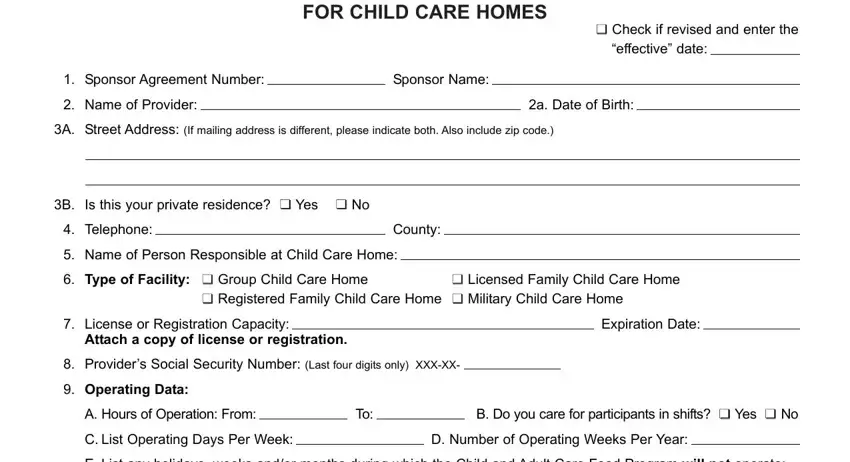
1. To start with, when completing the Dss Form 1606, start with the section that includes the subsequent fields:
2. Once your current task is complete, take the next step – fill out all of these fields - E List any holidays weeks andor, F Age Range of Enrolled Children, Meal Service, A cid Meals Claimed for, cid, cidcid Breakfast, cidcid AM, Supplement, cidcid Lunch, cidcid PM, Supplement, cidcid Supper, cidcid Evening Supplement, B Time of Meal Service, and Number of Children and Under with their corresponding information. Make sure to double check that everything has been entered correctly before continuing!
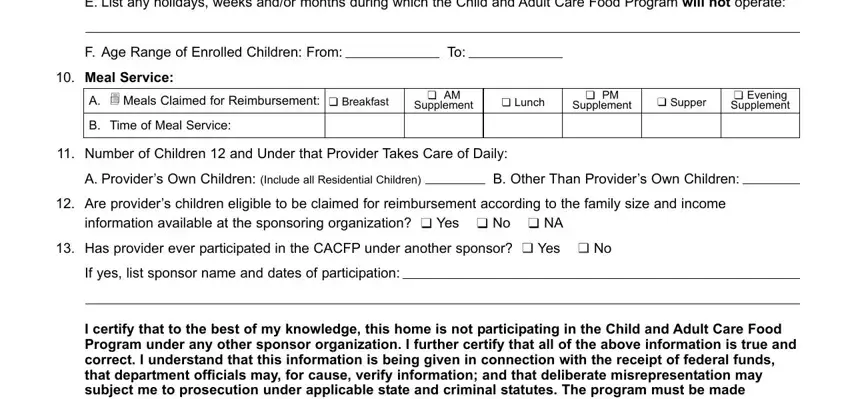
3. Completing I certify that to the best of my, Providers Signature, Sponsoring Organization, DSS Form MAY Edition of JUN is, Date, and Date is essential for the next step, make sure to fill them out in their entirety. Don't miss any details!

It's simple to make a mistake when completing your DSS Form MAY Edition of JUN is, thus make sure that you reread it prior to when you finalize the form.
Step 3: Right after proofreading the entries, press "Done" and you are done and dusted! After setting up afree trial account with us, you will be able to download Dss Form 1606 or email it without delay. The file will also be readily accessible in your personal account with all of your changes. At FormsPal.com, we do our utmost to be sure that all your information is stored secure.