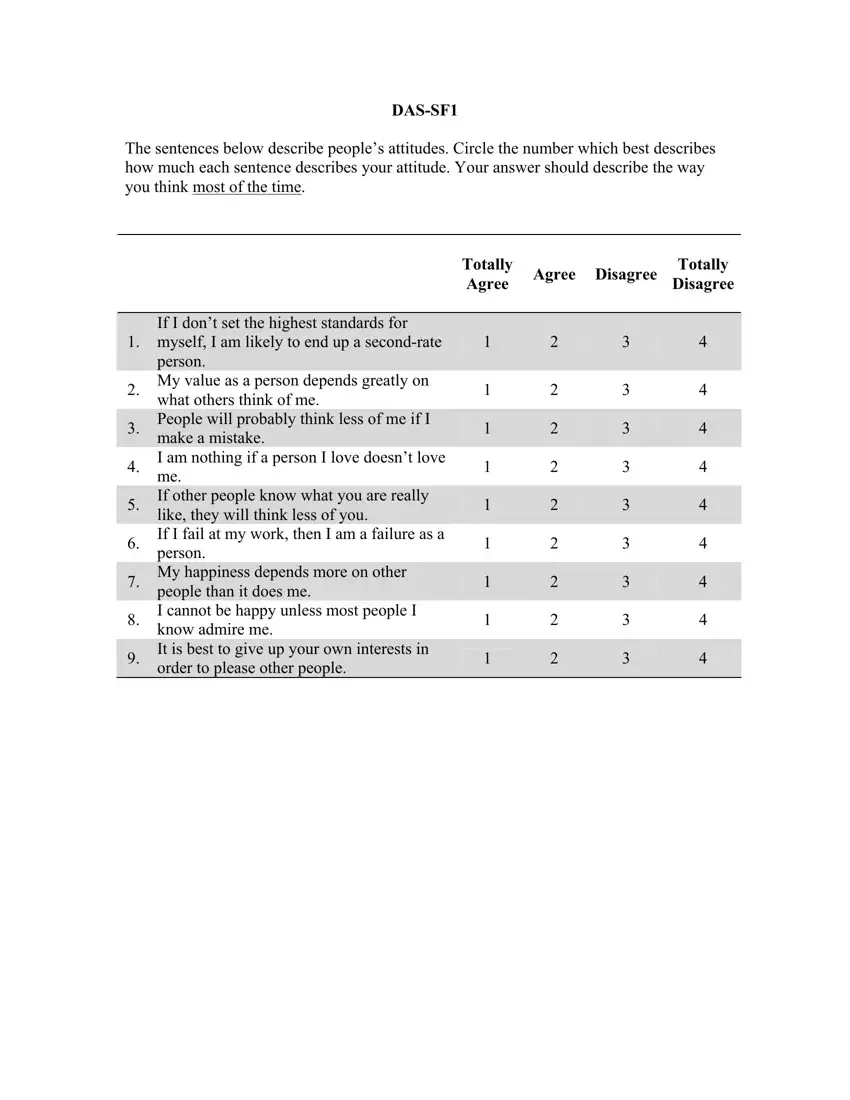
Understanding one's own attitudes and beliefs, especially when they are detrimental to one's mental health, is a crucial step in addressing and mitigating the effects of depression. The Dysfunctional Attitude Scale Forms, DAS-SF1 and DAS-SF2, serve this exact purpose by efficiently gauging negative cognition commonly associated with depression. Developed through rigorous research by Christopher G. Beevers, David R. Strong, and their colleagues, these short-form scales have demonstrated strong reliability and validity, offering a quick yet accurate method for assessing dysfunctional attitudes. These scales, consisting of carefully selected items that reflect rigid, perfectionist, and self-depreciating beliefs, are a testament to the advancements in psychological assessment. The scoring of these forms is designed to reflect the severity of dysfunctional attitudes, with higher scores indicating greater levels of dysfunctional thinking. By providing an efficient tool for the assessment of such attitudes among individuals with depression, these forms not only facilitate research and clinical work but also pave the way for targeted interventions, ultimately contributing to the improvement of mental health outcomes.
| Question | Answer |
|---|---|
| Form Name | Dtsfunctional Additude Scale |
| Form Length | 14 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 3 min 30 sec |
| Other names | dysfunctional attitude scale 40 item pdf, dysfunctional attitude scale 40 items pdf, das questionnaire, dysfunctional attitude scale quiz |
