


When using the online PDF editor by FormsPal, you can easily complete or change medicaid relationship familial right here. In order to make our editor better and less complicated to work with, we consistently work on new features, taking into consideration suggestions coming from our users. By taking a few easy steps, you'll be able to begin your PDF journey:
Step 1: Simply click the "Get Form Button" above on this webpage to launch our pdf file editing tool. There you'll find everything that is necessary to fill out your document.
Step 2: As you start the file editor, there'll be the document all set to be filled out. Other than filling in various blanks, you may also perform various other actions with the PDF, namely putting on your own text, editing the original textual content, adding graphics, signing the PDF, and a lot more.
This PDF form requires specific information to be entered, therefore be certain to take the time to type in exactly what is requested:
1. You need to complete the medicaid relationship familial properly, so be attentive while working with the parts including these specific blanks:
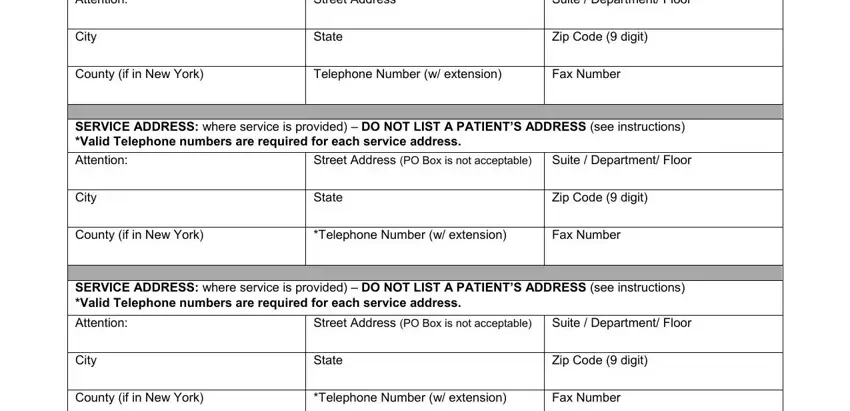
2. Just after filling out the last section, head on to the subsequent step and complete the necessary details in all these blanks - CORRESPONDENCE ADDRESS PO Box not, Suite Department Floor, City, State, Zip Code digit, County if in New York, Telephone Number w extension, Fax Number, SERVICE ADDRESS where service is, Street Address PO Box is not, Suite Department Floor, City, State, Zip Code digit, and County if in New York.
3. In this particular part, check out Name, NPI, Home Address Street, City State, Zip Code digits, SSN, Date of Birth, Ownership in Applicant if required, Name of Individual or Entity, of Ownership, NPI, Address Home Address if individual, City State, Zip Code digits, and SSN if indiv FEIN if entity. Each one of these are required to be completed with utmost precision.
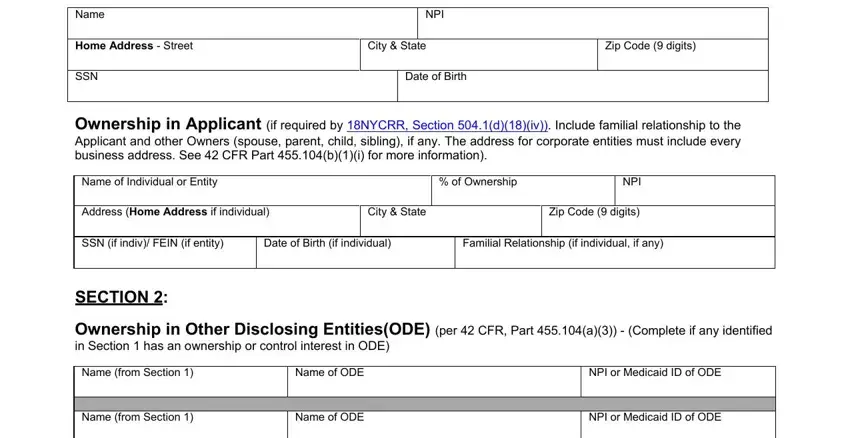
It is possible to get it wrong while filling out your Ownership in Applicant if required, so be sure to take another look before you finalize the form.
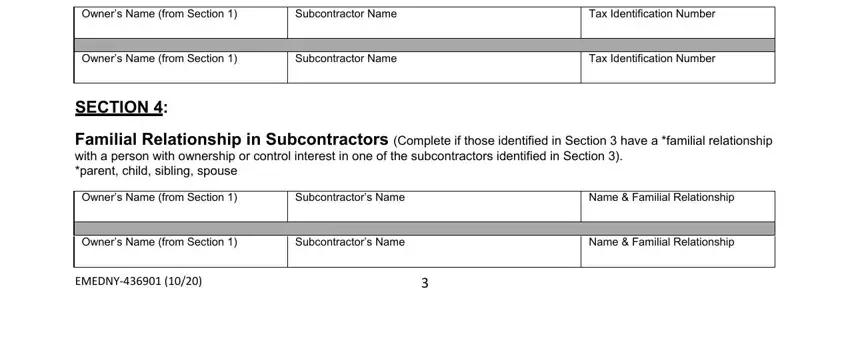
4. To move forward, the following stage involves filling out several empty form fields. Included in these are Owners Name from Section, Subcontractor Name, Tax Identification Number, Owners Name from Section, Subcontractor Name, Tax Identification Number, SECTION, Familial Relationship in, Owners Name from Section, Subcontractors Name, Name Familial Relationship, Owners Name from Section, Subcontractors Name, Name Familial Relationship, and EMEDNY, which are key to moving forward with this particular PDF.
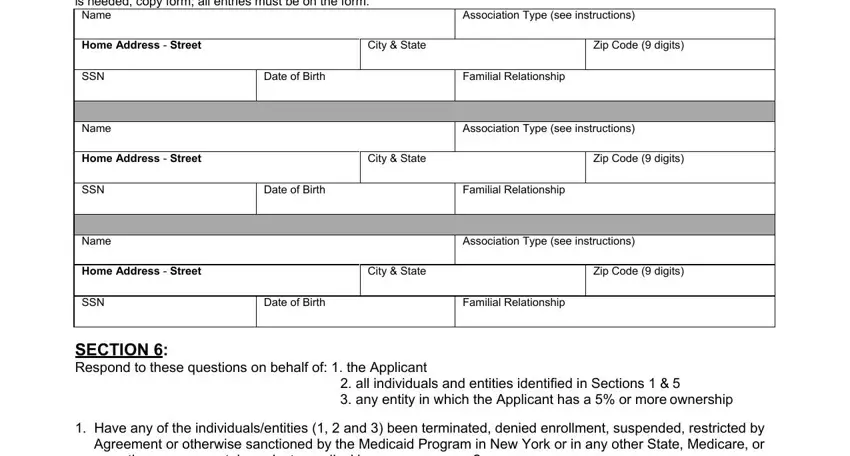
5. As you come near to the final sections of the document, you will find a couple extra things to do. In particular, Completion of all fields is, Name, Association Type see instructions, Home Address Street, City State, Zip Code digits, SSN, Name, Date of Birth, Familial Relationship, Association Type see instructions, Home Address Street, City State, Zip Code digits, and SSN must all be filled in.
Step 3: Prior to finalizing the form, it's a good idea to ensure that blanks have been filled out as intended. As soon as you establish that it's correct, press “Done." After creating a7-day free trial account at FormsPal, it will be possible to download medicaid relationship familial or email it directly. The document will also be available in your personal cabinet with your every change. Here at FormsPal.com, we strive to be sure that all your details are maintained secure.