
If you want to fill out ECG, you don't have to install any kind of software - simply use our PDF tool. Our tool is consistently evolving to present the very best user experience achievable, and that's thanks to our dedication to constant improvement and listening closely to user comments. It just takes several easy steps:
Step 1: First of all, access the pdf editor by clicking the "Get Form Button" in the top section of this page.
Step 2: With the help of this state-of-the-art PDF editor, you may accomplish more than merely fill in blank fields. Express yourself and make your documents seem great with custom textual content added, or modify the file's original input to perfection - all comes along with an ability to incorporate any type of graphics and sign the PDF off.
Filling out this document demands thoroughness. Ensure all necessary blanks are filled out accurately.
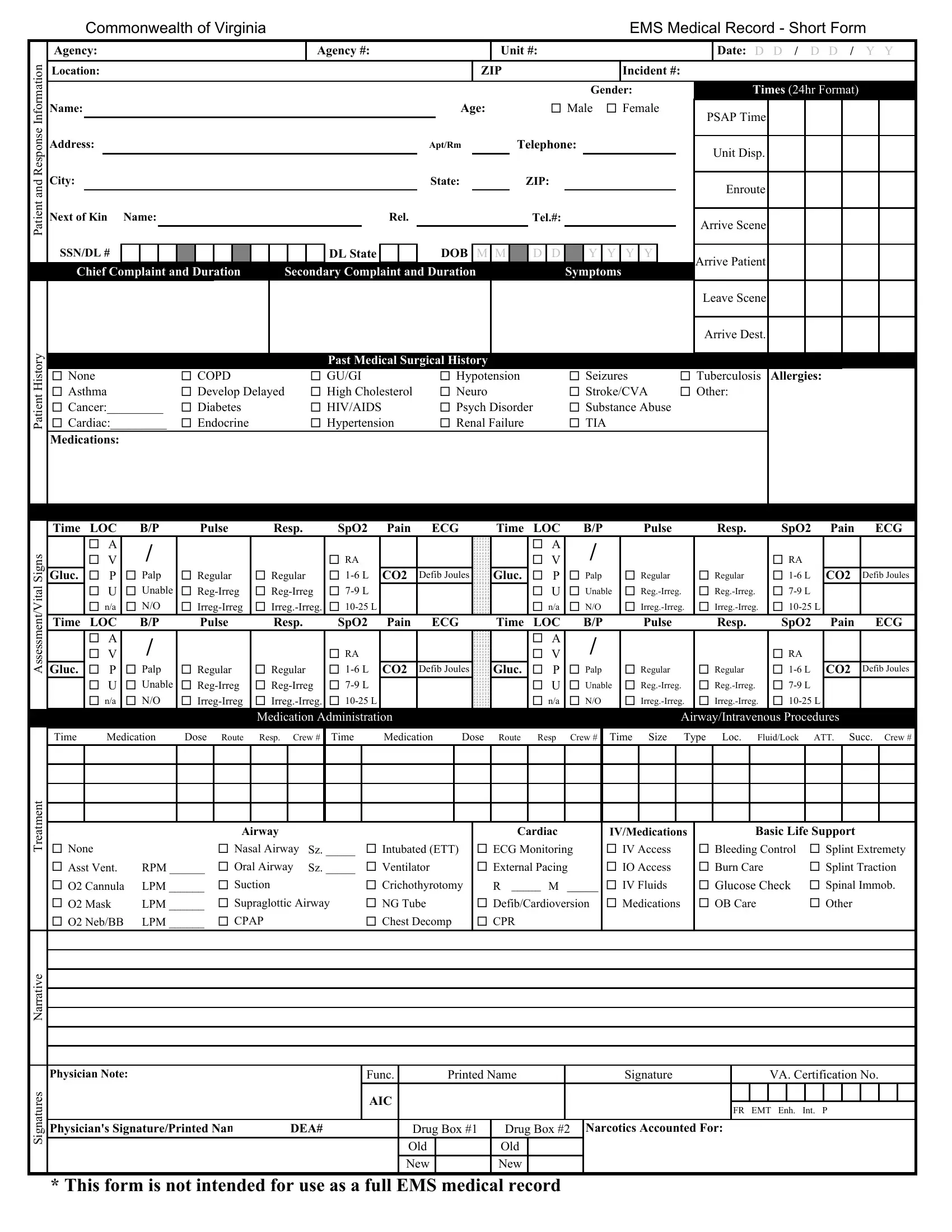
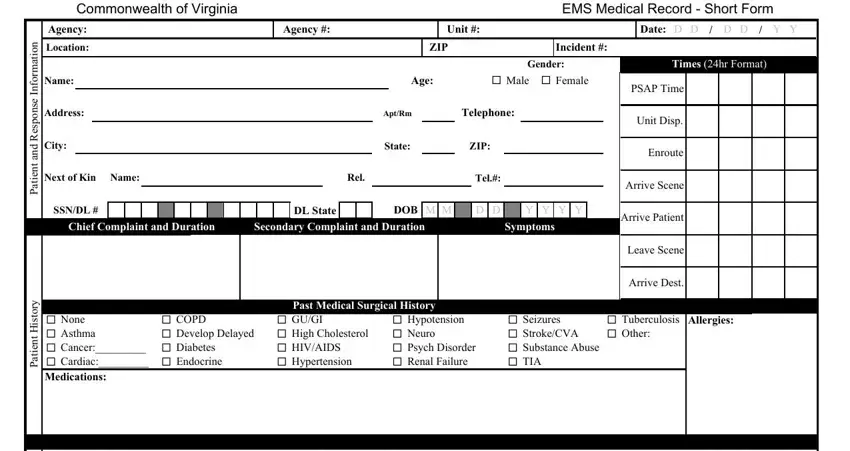
1. The ECG needs specific details to be inserted. Ensure the subsequent blank fields are finalized:
2. Now that this part is finished, you should insert the essential particulars in s n g i, l a t i, t n e m s s e s s A, t n e m t a e r T, e v i t a r r a N, Gluc, Time LOC A V P U na LOC A, Time, Gluc, Pulse, Resp, SpO, Pain, ECG, and Time so that you can progress further.
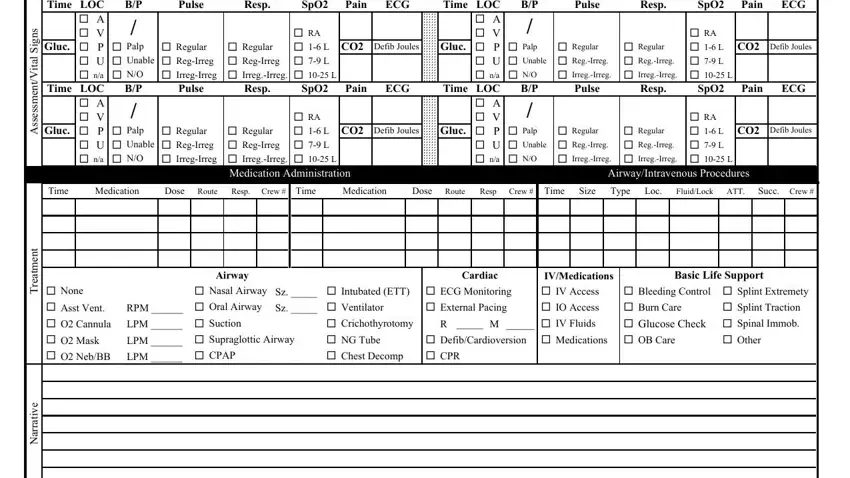
When it comes to e v i t a r r a N and t n e m t a e r T, be certain you get them right in this current part. Both of these are viewed as the most important fields in the file.
3. In this stage, review s e r u t a n g i S, Physician Note, Func, AIC, Printed Name, Signature, VA Certification No, FR EMT Enh Int P, Physicians SignaturePrinted Nam, DEA, Drug Box, Drug Box, Narcotics Accounted For, This form is not intended for use, and Old. These must be filled in with utmost accuracy.

Step 3: Prior to moving forward, check that form fields have been filled out right. As soon as you believe it's all good, click “Done." Get the ECG once you sign up for a free trial. Readily access the pdf document in your personal cabinet, with any edits and adjustments being automatically preserved! FormsPal offers safe document tools without data record-keeping or distributing. Be assured that your details are secure with us!