
Using PDF documents online is definitely simple with this PDF editor. Anyone can fill out ky commonwealth certificate immunization here painlessly. Our team is constantly working to enhance the tool and help it become much easier for clients with its many functions. Bring your experience to the next level with constantly developing and fantastic possibilities we provide! This is what you'll need to do to start:
Step 1: Just click the "Get Form Button" in the top section of this page to see our pdf form editor. Here you will find all that is needed to fill out your document.
Step 2: With the help of our advanced PDF editing tool, it is possible to accomplish more than just fill in forms. Express yourself and make your documents look great with customized textual content put in, or adjust the file's original content to excellence - all supported by an ability to add just about any graphics and sign the file off.
This PDF doc will require some specific information; to ensure accuracy, remember to take into account the guidelines listed below:
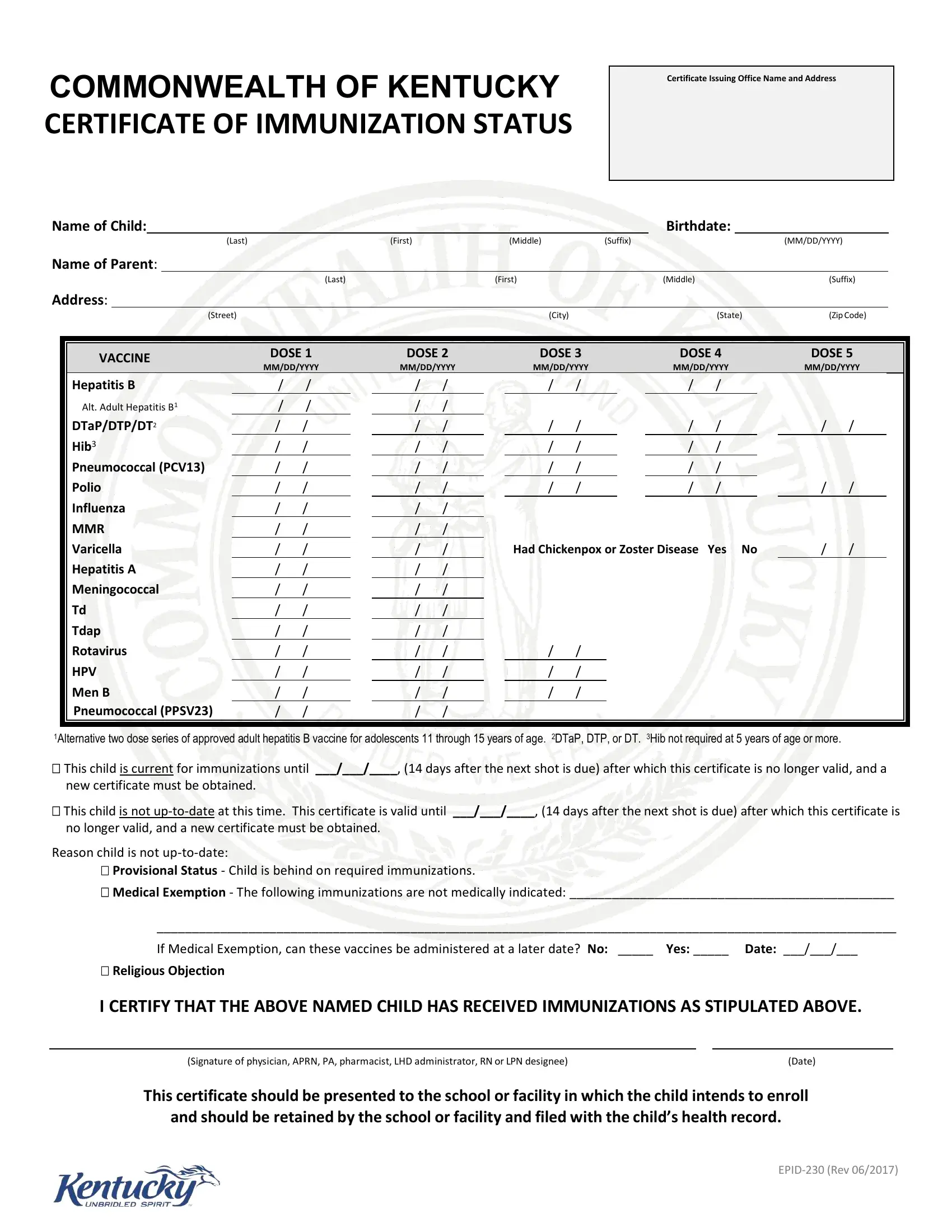
1. The ky commonwealth certificate immunization needs particular information to be typed in. Make certain the next blank fields are completed:
2. Immediately after the previous section is completed, go to enter the relevant details in these: Pneumococcal PCV, Polio, Influenza, MMR, Varicella, Hepatitis A, Meningococcal, Tdap, Rotavirus, HPV, Men B Pneumococcal PPSV, Had Chickenpox or Zoster Disease, Alternative two dose series of, This child is current for, and new certificate must be obtained.
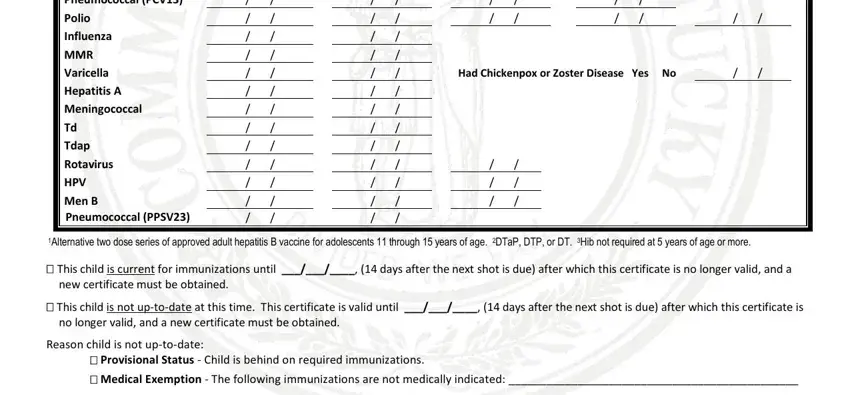
Concerning Influenza and Meningococcal, make sure that you don't make any errors here. The two of these could be the most important ones in the file.
3. The third stage is usually simple - fill in every one of the form fields in If Medical Exemption can these, Religious Objection, I CERTIFY THAT THE ABOVE NAMED, Signature of physician APRN PA, Date, This certificate should be, and should be retained by the, and EPID Rev to conclude this part.
Step 3: Right after proofreading your fields and details, press "Done" and you're good to go! Sign up with FormsPal now and instantly obtain ky commonwealth certificate immunization, all set for download. All modifications you make are saved , letting you modify the file further if required. At FormsPal, we endeavor to make sure all of your information is kept private.