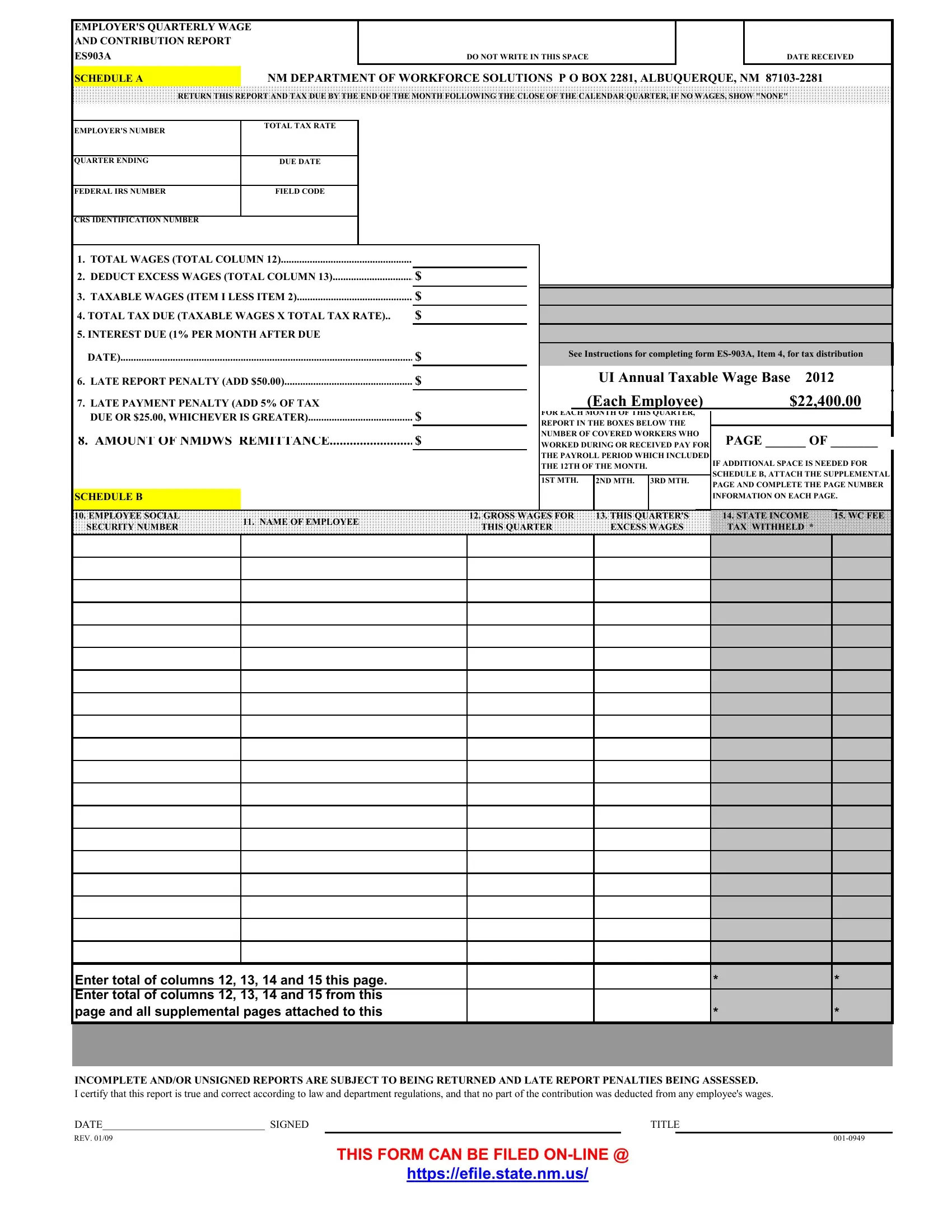
In the tapestry of business operations, financial transparency and adherence to regulatory requirements form the core of organizational integrity. Among the myriad forms and reports that businesses must navigate, the Employer's Quarterly Wage and Contribution Report, known as the ES903A, holds a pivotal role, particularly in the realm of employment taxes within New Mexico. This form serves as a critical conduit for employers to report wages paid, contributions due, and other pertinent payroll information to the New Mexico Department of Workforce Solutions. The ES903A form is structured to encapsulate a comprehensive snapshot of an employer's quarterly financial obligations regarding employee wages, including total wages paid, deductions for excess wages, taxable wages, total tax due, and any penalties or interest incurred for late submissions. Additionally, the form demands specifics about each worker, such as social security number, name, gross wages for the quarter, state income tax withheld, and workers' compensation fees, all aimed at fostering a transparent record-keeping environment. Employers are mandated to submit this documentation by the end of the month following the close of a calendar quarter, ensuring that the wheels of fiscal responsibility and compliance turn smoothly within the state's economic structure. Beyond mere compliance, the ES903A form stands as a testament to the essential dialogue between businesses and regulatory bodies, serving to fortify worker protections and contribute to the overall health of New Mexico's labor market.
| Question | Answer |
|---|---|
| Form Name | Es903A Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | es903a form fillable, es903a, nm es903a, what is a es903a form |
EMPLOYER'S QUARTERLY WAGE |
|
|
|
|
|
AND CONTRIBUTION REPORT |
|
|
|
|
|
ES903A |
|
DO NOT WRITE IN THIS SPACE |
|
DATE RECEIVED |
|
SCHEDULE A |
|
NM DEPARTMENT OF WORKFORCE SOLUTIONS P O BOX 2281, ALBUQUERQUE, NM |
|||
RETURN THIS REPORT AND TAX DUE BY THE END OF THE MONTH FOLLOWING THE CLOSE OF THE CALENDAR QUARTER, IF NO WAGES, SHOW "NONE"
EMPLOYER'S NUMBER
TOTAL TAX RATE
QUARTER ENDING
DUE DATE
FEDERAL IRS NUMBER
FIELD CODE
CRS IDENTIFICATION NUMBER
1. |
TOTAL WAGES (TOTAL COLUMN 12) |
|
|
|
|
2. |
DEDUCT EXCESS WAGES (TOTAL COLUMN 13) |
$ |
|
|
|
3. |
TAXABLE WAGES (ITEM I LESS ITEM 2) |
$ |
4. TOTAL TAX DUE (TAXABLE WAGES X TOTAL TAX RATE).. |
$ |
|
5. INTEREST DUE (1% PER MONTH AFTER DUE |
|
|
|
DATE) |
$ |
6. |
LATE REPORT PENALTY (ADD $50.00) |
$ |
7. |
LATE PAYMENT PENALTY (ADD 5% OF TAX |
|
|
DUE OR $25.00, WHICHEVER IS GREATER) |
$ |
8. AMOUNT OF NMDWS REMITTANCE |
$ |
|
SCHEDULE B
See Instructions for completing form
UI Annual Taxable Wage Base 2012
|
(Each Employee) |
$22,400.00 |
|
|
||||
FOR EACH MONTH OF THIS QUARTER, |
|
|
|
|
||||
|
|
|
|
|||||
REPORT IN THE BOXES BELOW THE |
|
|
|
|
||||
NUMBER OF COVERED WORKERS WHO |
PAGE ______ OF _______ |
|
||||||
|
||||||||
WORKED DURING OR RECEIVED PAY FOR |
|
|||||||
THE PAYROLL PERIOD WHICH INCLUDED |
|
|
|
|
||||
THE 12TH OF THE MONTH. |
IF ADDITIONAL SPACE IS NEEDED FOR |
|
||||||
|
|
|
|
|||||
|
|
|
|
|
SCHEDULE B, ATTACH THE SUPPLEMENTAL |
|
||
1ST MTH. |
2ND MTH. |
3RD MTH. |
PAGE AND COMPLETE THE PAGE NUMBER |
|
||||
|
|
|
|
|
|
|||
|
|
|
|
|
INFORMATION ON EACH PAGE. |
|
||
|
|
|
|
|
|
|
|
|
10. EMPLOYEE SOCIAL |
11. NAME OF EMPLOYEE |
12. GROSS WAGES FOR |
13. THIS QUARTER'S |
14. STATE INCOME |
15. WC FEE |
SECURITY NUMBER |
THIS QUARTER |
EXCESS WAGES |
TAX WITHHELD * |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Enter total of columns 12, 13, |
14 and 15 this page. |
|
|
* |
* |
|
Enter total of columns 12, 13, |
14 and 15 from this |
|
|
|
|
|
page and all supplemental pages attached to this |
|
|
* |
* |
||
|
|
|
|
|
|
|
INCOMPLETE AND/OR UNSIGNED REPORTS ARE SUBJECT TO BEING RETURNED AND LATE REPORT PENALTIES BEING ASSESSED.
I certify that this report is true and correct according to law and department regulations, and that no part of the contribution was deducted from any employee's wages.
DATE______________________________ SIGNED |
|
TITLE |
|
REV. 01/09 |
|
|
|
THIS FORM CAN BE FILED