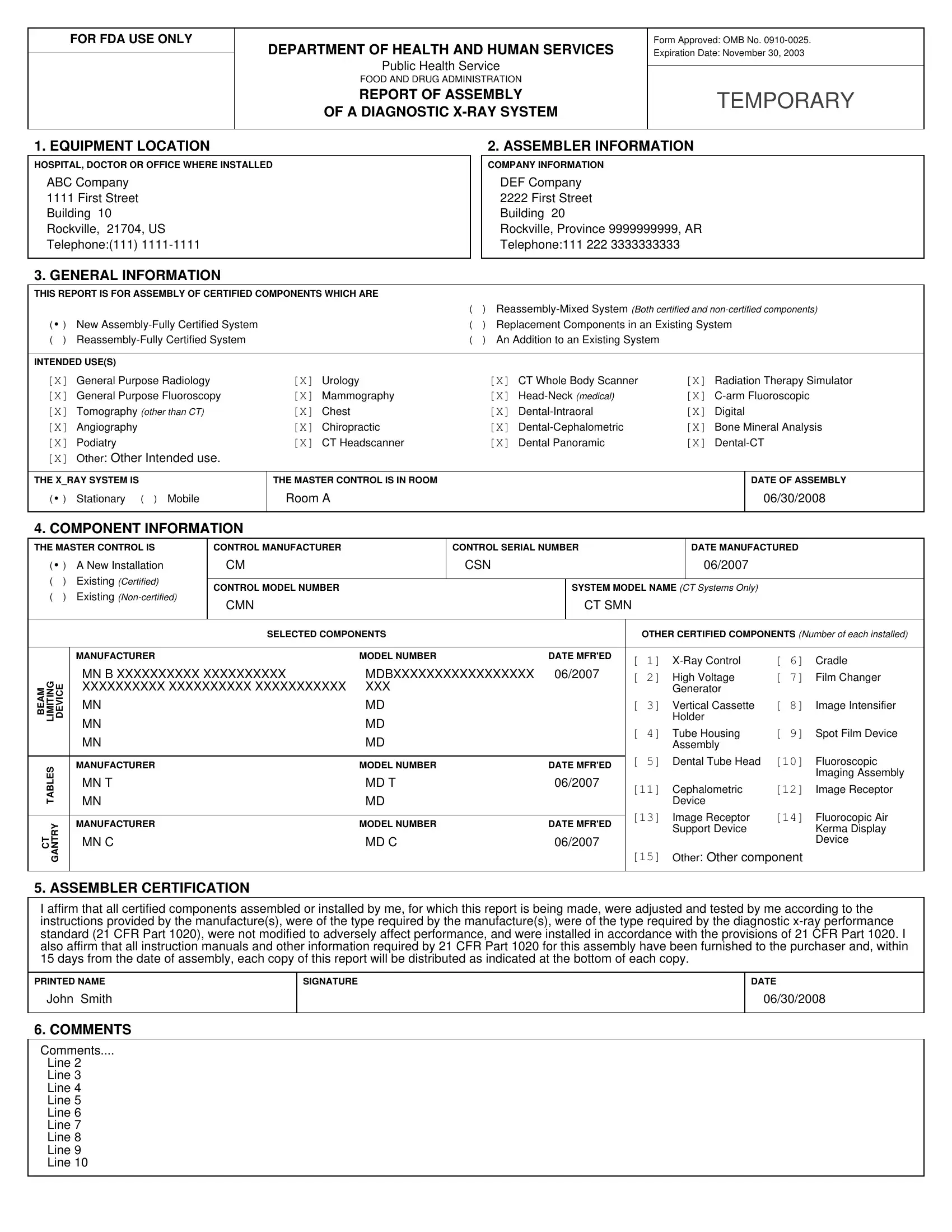
The FDA 2579 form, officially known as the "Report of Assembly of a Diagnostic X-Ray System," plays a crucial role in ensuring the safety and compliance of diagnostic x-ray equipment throughout the United States. Mandated by the Department of Health and Human Services and the Food and Drug Administration, this form is a necessary component of the regulatory framework that oversees the assembly, installation, and proper functioning of x-ray systems. Its comprehensive nature requires detailed information, including the location where the equipment is installed, assembler's details, general information on the system's intended use, component specifics, and certification by the assembler that all parts meet the diagnostic x-ray performance standards as set out in 21 CFR Part 1020. The form also documents the types of systems assembled, whether they are fully certified systems, reassemblies, replacements, or additions, and covers a broad spectrum of medical applications from general radiology to more specialized fields such as mammography and dental cephalometry. An assembler's affirmation signifies that all components were adjusted, tested, not modified adversely, and installed according to federal standards, ensuring that each x-ray system assembled contributes to safe and effective medical diagnostics. This rigorous documentation process, underscored by the FDA 2579 form, epitomizes the extensive measures taken to protect public health by ensuring diagnostic x-ray equipment adheres to the highest safety standards.
| Question | Answer |
|---|---|
| Form Name | Fda 2579 Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | form fda 2579, 2579, fda form 2579, fda 2579 form pdf printable |
