

It really is very easy to fill in the el2 physical form. Our PDF editor was meant to be help you complete any PDF efficiently. These are the basic actions to take:
Step 1: The very first step is to hit the orange "Get Form Now" button.
Step 2: The file editing page is now available. Include text or enhance existing information.
If you want to prepare the template, type in the content the platform will request you to for each of the following sections:
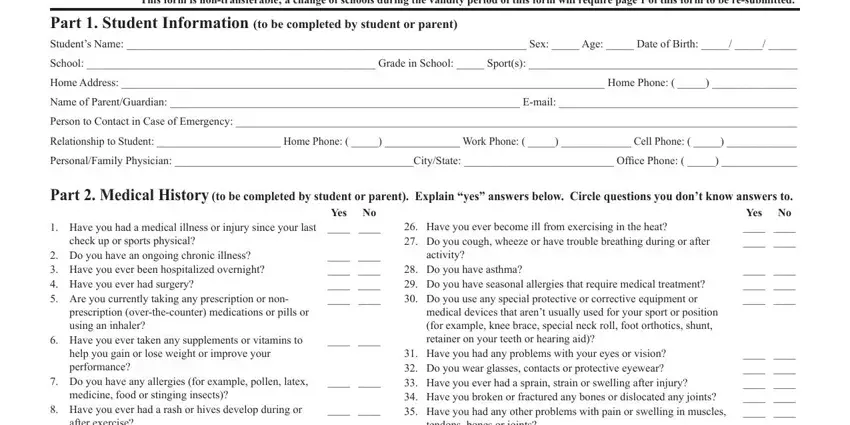
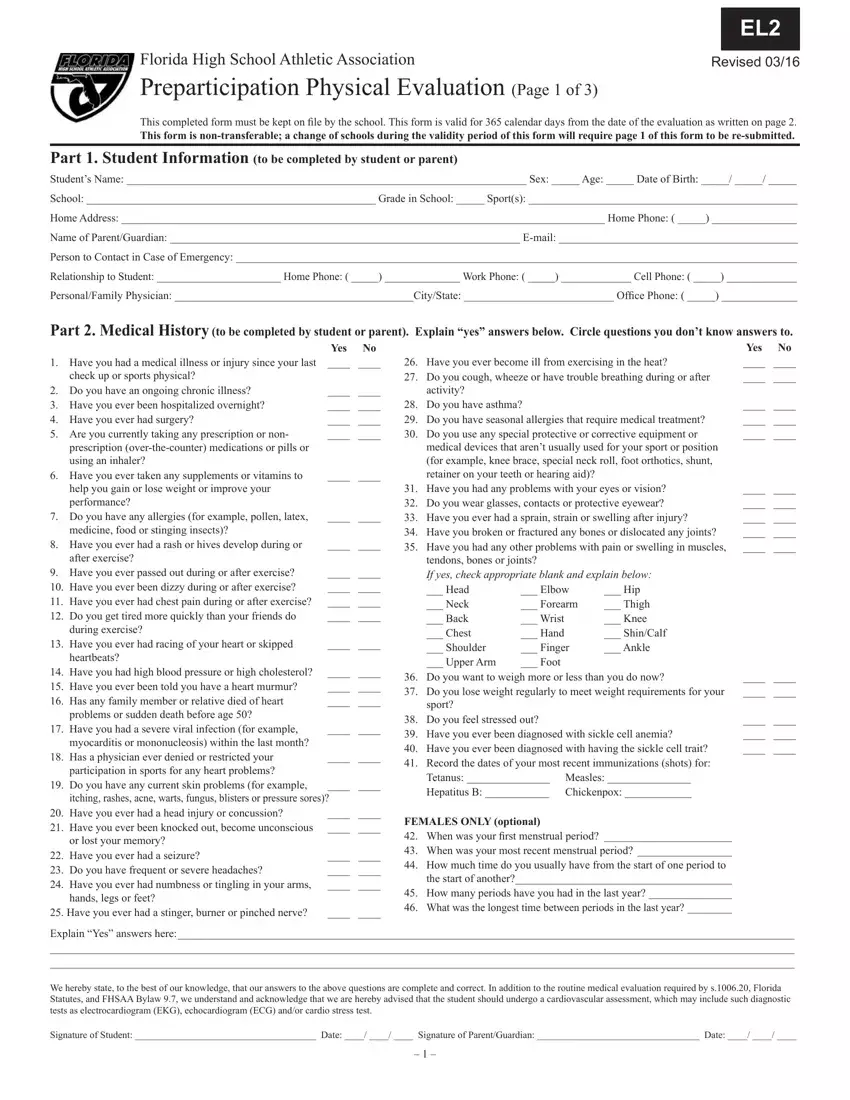
Type in the details in the after exercise, Have you ever passed out during, during exercise, Have you ever had racing of your, heartbeats, Have you had high blood pressure, problems or sudden death before, Have you had a severe viral, Do you have any current skin, itching rashes acne warts fungus, Have you ever had a head injury, or lost your memory, Have you ever had a seizure Do, hands legs or feet, and Have you ever had a stinger field.
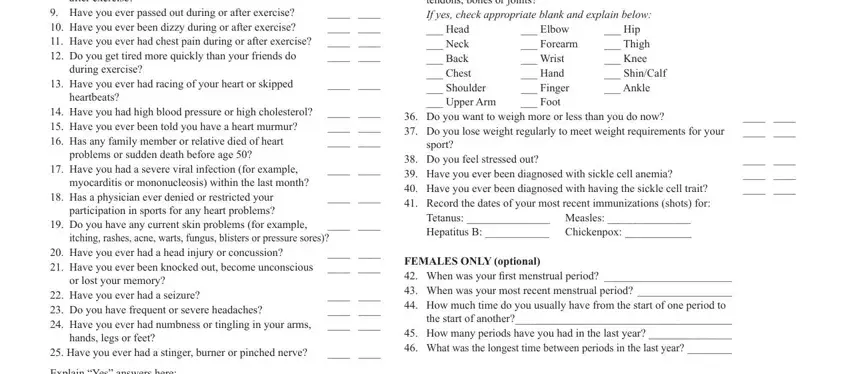
Write any details you may need in the area Explain Yes answers here, We hereby state to the best of our, and Signature of Student Date.

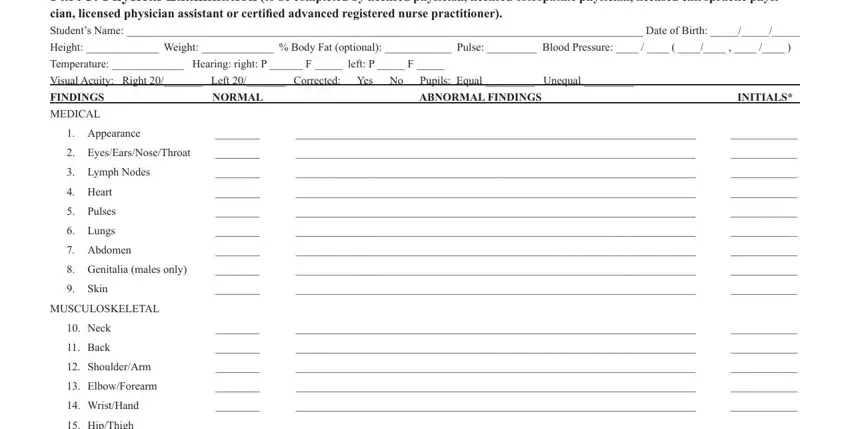
Indicate the rights and responsibilities of the sides inside the box Part Physical Examination to be, Height Weight Body Fat optional, Temperature Hearing right P F, Visual Acuity Right Left, FINDINGS, MEDICAL, NORMAL, ABNORMAL FINDINGS, INITIALS, Appearance, EyesEarsNoseThroat, Lymph Nodes, Heart, Pulses, and Lungs.
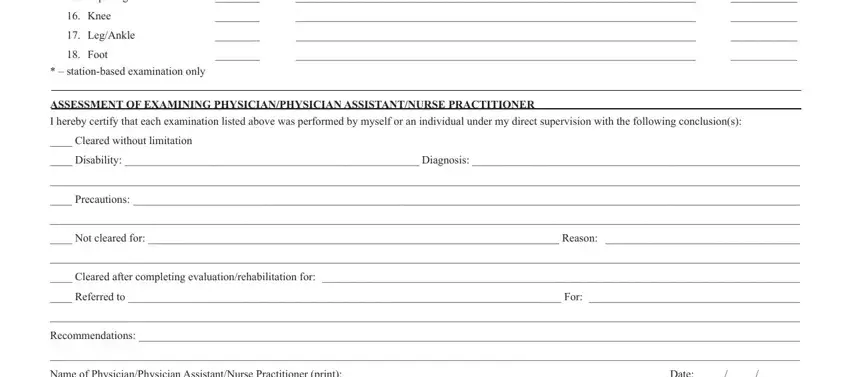
End by taking a look at all these fields and filling them in as required: HipThigh, Knee, LegAnkle, Foot, stationbased examination only, ASSESSMENT OF EXAMINING, I hereby certify that each, Cleared without limitation, Disability Diagnosis, Precautions, Not cleared for Reason, Cleared after completing, Referred to For, Recommendations, and Name of PhysicianPhysician.
Step 3: Hit the button "Done". The PDF document is available to be exported. You can easily upload it to your laptop or email it.
Step 4: Make duplicates of your form - it will help you stay away from potential concerns. And don't worry - we are not meant to display or see your data.
