We've used the hard work of our best software engineers to make the PDF editor you are about to benefit from. Our application will enable you to complete the universal medication form form easily and don’t waste valuable time. Everything you need to undertake is comply with these particular easy recommendations.
Step 1: Click the button "Get Form Here".
Step 2: You can now change your universal medication form. This multifunctional toolbar makes it possible to add, remove, modify, and highlight text as well as carry out other commands.
These sections are what you will have to prepare to get the prepared PDF form.
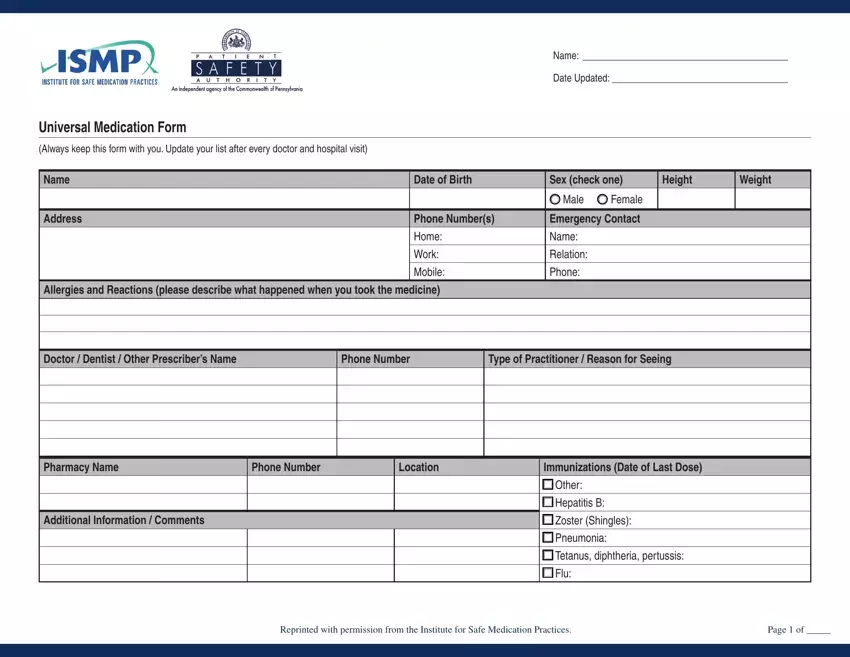
Provide the requested particulars in the Doctor Dentist Other Prescribers, Phone Number, Type of Practitioner Reason for, Pharmacy Name, Phone Number, Location, Immunizations Date of Last Dose, Additional Information Comments, Other, Hepatitis B, Zoster Shingles, Pneumonia, Tetanus diphtheria pertussis, Flu, and Reprinted with permission from the section.
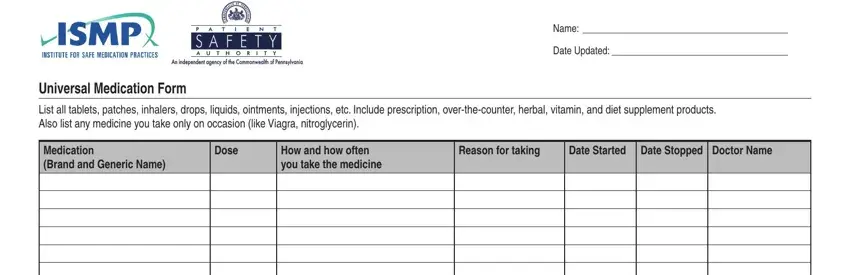
It's important to provide certain data in the section Name, Date Updated, Universal Medication Form, List all tablets patches inhalers, Medication Brand and Generic Name, Dose, How and how often you take the, Reason for taking, Date Started, and Date Stopped Doctor Name.
The field will be the place to insert the rights and responsibilities of both sides.
Finish by checking all these sections and filling them in accordingly: Check here if additional pages of, Reprinted with permission from the, and Page of.

Step 3: Hit the Done button to ensure that your finished document is available to be exported to any type of gadget you choose or mailed to an email you specify.
Step 4: It may be easier to maintain duplicates of the file. You can rest assured that we are not going to distribute or read your information.
