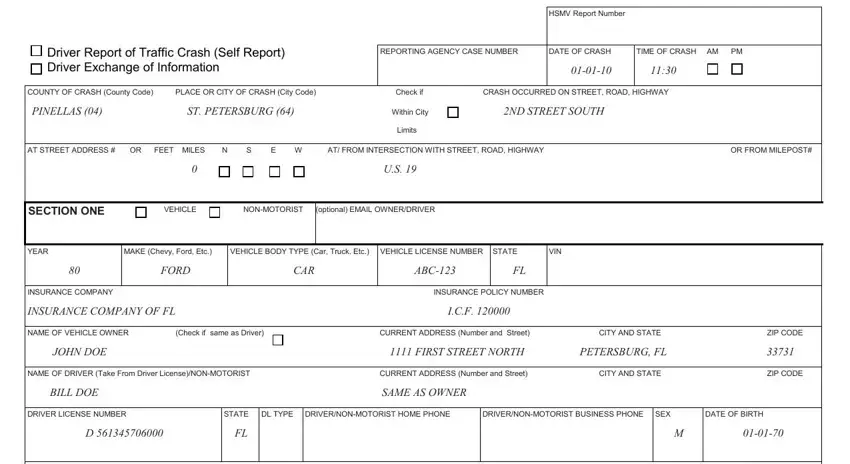
 Driver Report of Traffic Crash (Self Report)
Driver Report of Traffic Crash (Self Report) 
 Driver Exchange of Information
Driver Exchange of Information
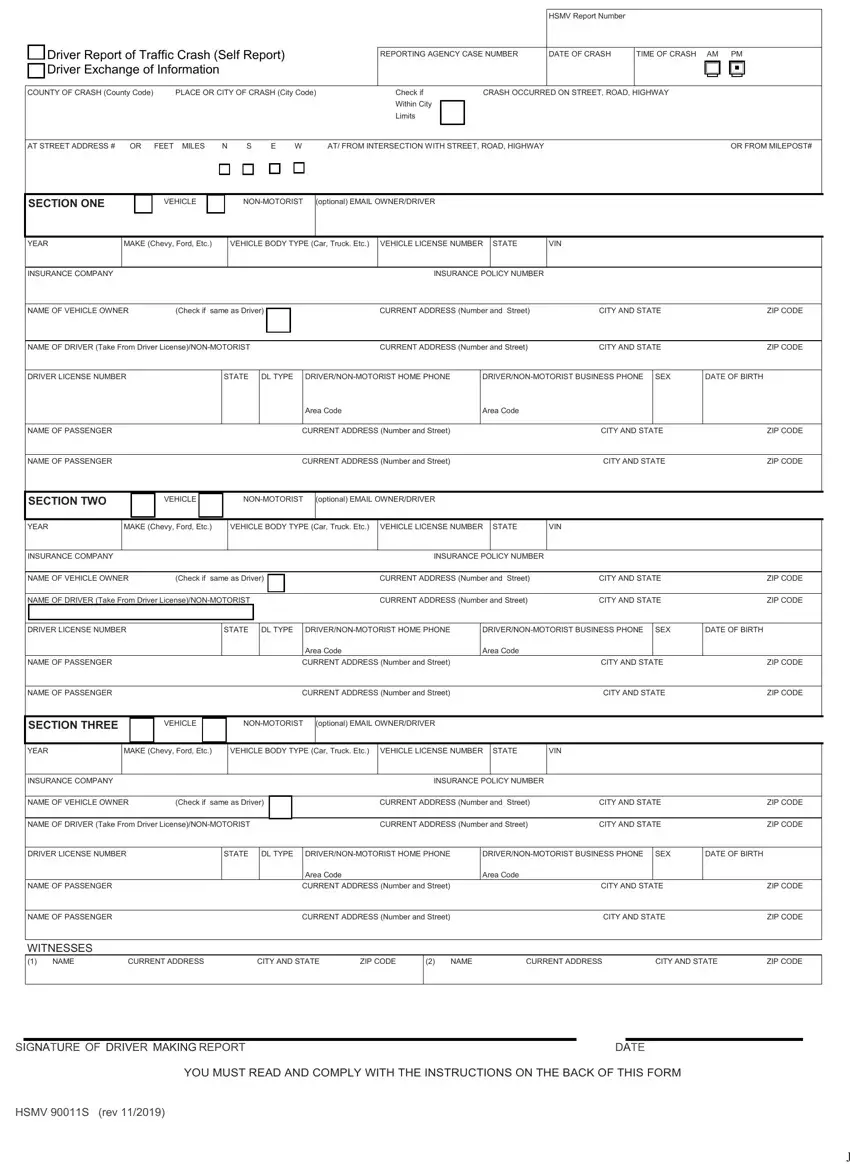
Completing the Florida Traffic Crash Report form guarantees that all essential traffic incident information is correctly recorded. This documentation is essential for insurance claims and legal matters, as well as for adhering to state laws that might mandate a report for accidents with property damage, injuries, or fatalities. Here is a detailed guide to help you fill out this form using our PDF editor.
1. Basic Crash Information
Please fill in the details of the crash, including the HSMV report number, date and time of the crash, and the county and city where the crash occurred. If the crash happened within city limits, ensure you check the box.
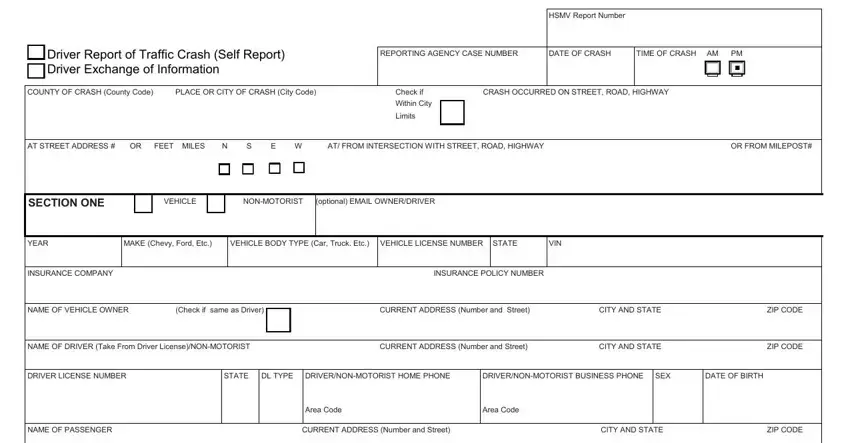
2. Document the Crash Location
Provide the specific location of the crash. This includes the street, road, or highway name and any pertinent details like the address number, miles or feet from an intersection, and direction (north, south, east, or west).
3. Vehicle and Driver Information
For each vehicle involved, input the year, make, model, body type, license number, state, and VIN. Also, provide insurance details, including the company name and policy number. Repeat this step for all vehicles involved in the crash.
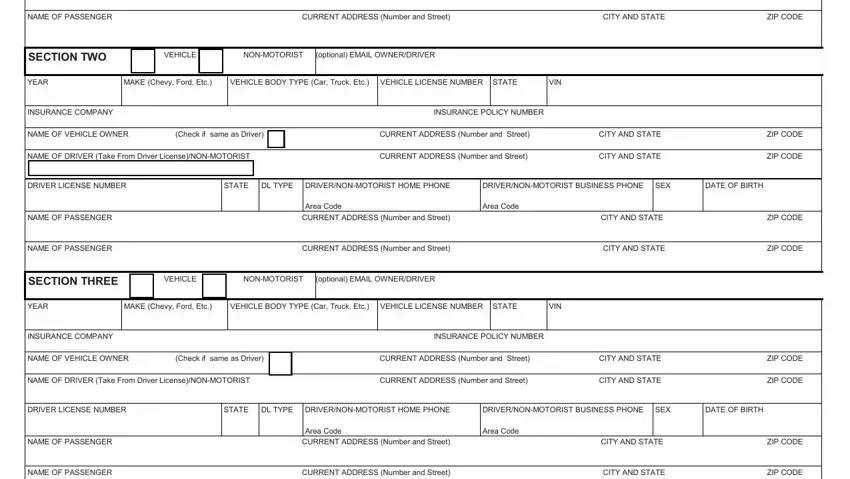
4. Personal Information for All Parties
Record the names, current addresses, states, ZIP codes, driver’s license numbers, and contact information for all drivers, passengers, and non-motorists involved. Specify their roles and if any injuries were sustained.
5. Describe the Accident
Provide a narrative description of how the crash occurred. This section should include all relevant details explaining the sequence of events leading to the accident. If the platform allows, you can also upload or draw a diagram of the accident scene.
6. Witness Information
If there were witnesses to the crash, enter their names, addresses, and contact information. This data can be crucial for insurance and legal purposes.
7. Review and Submit
Before submitting, review all the information entered for accuracy. Once confirmed, follow the instructions for submission, which may include options to email or mail the report to the FLHSMV.
