


Creating forms together with our PDF editor is more straightforward when compared with anything. To enhance flu vaccine paperwork the file, you'll find nothing you will do - basically stick to the actions below:
Step 1: Hit the button "Get form here" to open it.
Step 2: You're now on the document editing page. You can edit, add information, highlight particular words or phrases, insert crosses or checks, and add images.
The following parts will compose the PDF document that you will be filling in:
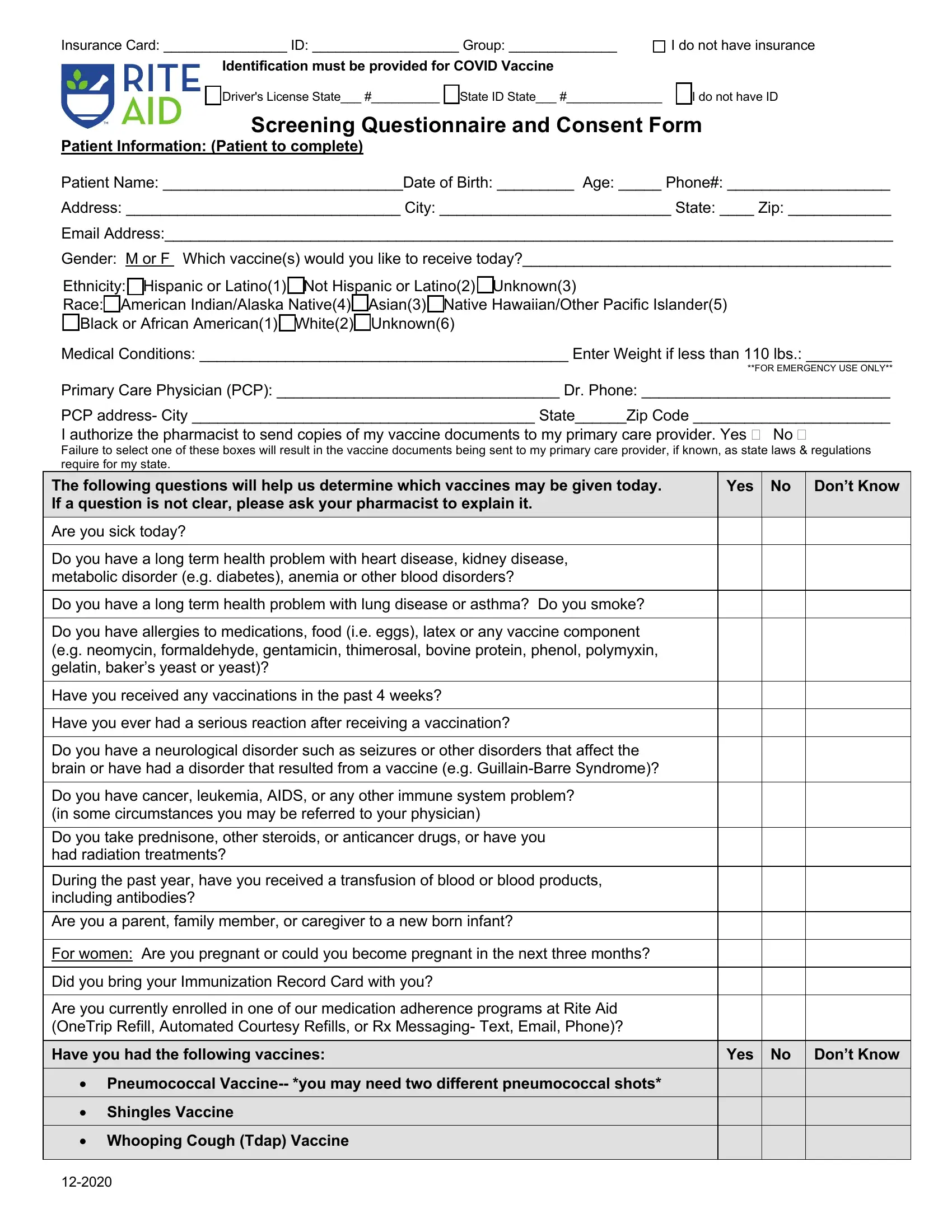
Provide the appropriate data in The following questions will help, Yes No Dont Know, Are you sick today, Do you have a long term health, Do you have a long term health, Do you have allergies to, Have you received any vaccinations, Have you ever had a serious, Do you have a neurological, Do you have cancer leukemia AIDS, and During the past year have you field.

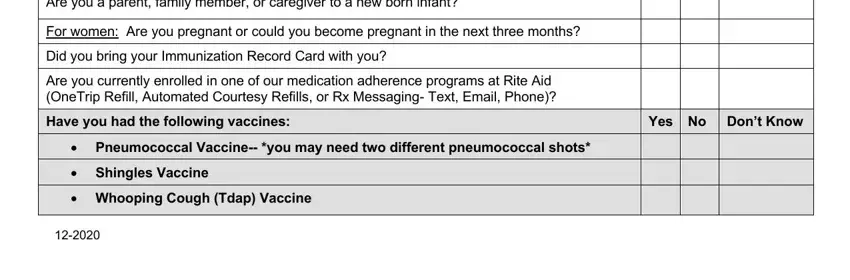
You'll have to write particular details inside the section During the past year have you, For women Are you pregnant or, Did you bring your Immunization, Are you currently enrolled in one, Have you had the following vaccines, Yes No Dont Know, Pneumococcal Vaccine you may need, Shingles Vaccine, and Whooping Cough Tdap Vaccine.
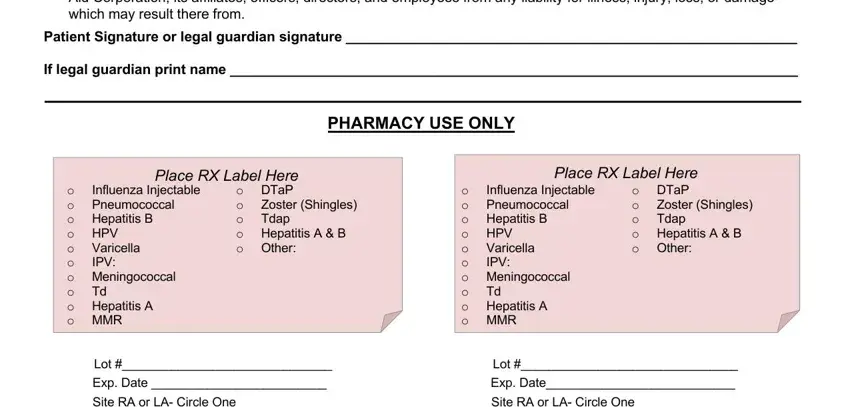
The I acknowledge that if my insurance, Patient Signature or legal, If legal guardian print name, PHARMACY USE ONLY, Place RX Label Here, Place RX Label Here, Zoster Shingles Tdap, o DTaP o o o Hepatitis A B o Other, Influenza Injectable Pneumococcal, Varicella IPV, o o o Hepatitis B o HPV o o o, Zoster Shingles Tdap, o DTaP o o o Hepatitis A B o Other, Influenza Injectable Pneumococcal, and Varicella IPV section can be used to indicate the rights and responsibilities of both sides.
Finish by reviewing the next fields and completing the appropriate particulars: Clinic Yes No, Signature of pharmacist who, License NPI Date, and Signature of Certified Immunizing.
Step 3: If you're done, click the "Done" button to export the PDF file.
Step 4: It could be easier to prepare copies of the file. You can rest easy that we are not going to reveal or read your particulars.