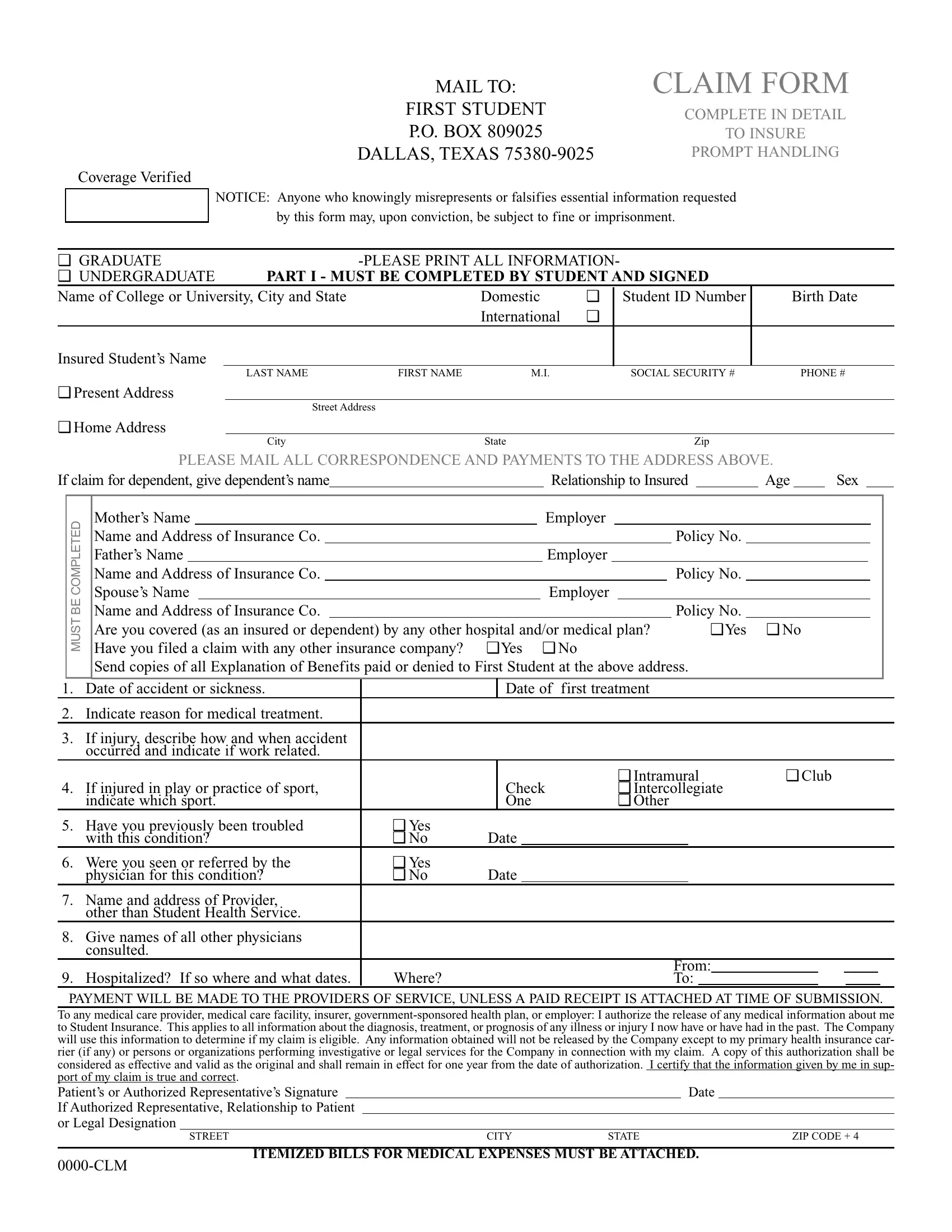
Submitting a claim for coverage can often seem like a daunting process, but understanding the requirements and details of forms like the 0000 Clm form can simplify the experience significantly. This particular form is essential for students needing to claim medical expenses through their insurance, requiring comprehensive information to ensure prompt and accurate handling. Sent to a designated address in Dallas, Texas, the form calls for meticulous detail from the student, including personal identification, the nature of the illness or injury, and information concerning other insurance coverage if applicable. Additionally, the form includes stern warnings against misrepresenting or falsifying information, highlighting the seriousness with which the claim is processed. It is designed to be filled out by both undergraduate and graduate students, with sections dedicated to capturing the student’s status, detailed personal information, and specifics about the medical treatment or incident leading to the claim. Furthermore, the form outlines a transparent process for where payments will be directed and requires authorization for the release of medical information, emphasizing the importance of providing accurate and truthful information to facilitate a smooth claim process. A thorough completion and understanding of this form can lead to more expedient claims handling, making it crucial for students to fill it out with great care and precision.
| Question | Answer |
|---|---|
| Form Name | Form 0000 Clm |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | Prescription_Cl aim_Form psi international student health insurance form |
MAIL TO: |
CLAIM FORM |
FIRST STUDENT |
COMPLETE IN DETAIL |
|
|
P.O. BOX 809025 |
TO INSURE |
DALLAS, TEXAS |
PROMPT HANDLING |
Coverage Verified
NOTICE: Anyone who knowingly misrepresents or falsifies essential information requested
by this form may, upon conviction, be subject to fine or imprisonment.
❑ GRADUATE |
|
|
||||
❑ UNDERGRADUATE |
PART I - MUST BE COMPLETED BY STUDENT AND SIGNED |
|
||||
Name of College or University, City and State |
|
Domestic |
❑ |
Student ID Number |
Birth Date |
|
|
|
|
International |
❑ |
|
|
Insured Student’s Name |
|
|
|
|
|
|
|
LAST NAME |
FIRST NAME |
M.I. |
|
SOCIAL SECURITY # |
PHONE # |
❑ Present Address
Street Address
❑Home Address
|
|
|
|
|
|
City |
|
State |
|
|
|
|
|
|
Zip |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
PLEASE MAIL ALL CORRESPONDENCE AND PAYMENTS TO THE ADDRESS ABOVE. |
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||
If claim for dependent, give dependent’s name |
|
|
|
|
|
|
Relationship to Insured |
Age |
Sex |
||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
COMPLETED |
|
Mother’s Name |
|
|
|
|
|
|
|
Employer |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
Name and Address of Insurance Co. |
|
|
|
|
|
|
|
|
|
|
|
|
|
Policy No. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
Father’s Name |
|
|
|
|
|
|
|
Employer |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
Name and Address of Insurance Co. |
|
|
|
|
|
|
|
|
|
|
|
|
|
Policy No. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
BE |
|
Spouse’s Name |
|
|
|
|
|
|
|
Employer |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
Name and Address of Insurance Co. |
|
|
|
|
|
|
|
|
|
|
|
|
|
Policy No. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
MUST |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
Are you covered (as an insured or dependent) by any other hospital and/or medical plan? |
|
|
|
❑ Yes |
❑ No |
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||
|
|
|
Have you filed a claim with any other insurance company? |
❑ Yes ❑ No |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
|
|
|
Send copies of all Explanation of Benefits paid or denied to First Student at the above address. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
1. |
Date of accident or sickness. |
|
|
Date of |
first treatment |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
2. |
Indicate reason for medical treatment. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
3. |
If injury, describe how and when accident |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
occurred and indicate if work related. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
❑ Intramural |
❑ Club |
|
|
|
|
|
|
|
|
|
|||||||||||
4. |
If injured in play or practice of sport, |
|
|
Check |
|
|
❑ Intercollegiate |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||
|
|
indicate which sport. |
|
|
One |
|
|
❑ Other |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
5. |
Have you previously been troubled |
❑ Yes |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
with this condition? |
❑ No |
Date |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
6. |
Were you seen or referred by the |
❑ Yes |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
physician for this condition? |
❑ No |
Date |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
7. |
Name and address of Provider, |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
other than Student Health Service. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
8. |
Give names of all other physicians |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
consulted. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
From: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
9. |
Hospitalized? If so where and what dates. |
Where? |
|
|
|
|
|
|
|
|
|
|
|
To: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
PAYMENT WILL BE MADE TO THE PROVIDERS OF SERVICE, UNLESS A PAID RECEIPT IS ATTACHED AT TIME OF SUBMISSION.
To any medical care provider, medical care facility, insurer,
Patient’s or Authorized Representative’s Signature |
|
|
|
Date |
|
|
If Authorized Representative, Relationship to Patient |
|
|
|
|
||
or Legal Designation |
|
|
|
|
||
|
STREET |
CITY |
STATE |
|
ZIP CODE + 4 |
|
ITEMIZED BILLS FOR MEDICAL EXPENSES MUST BE ATTACHED.