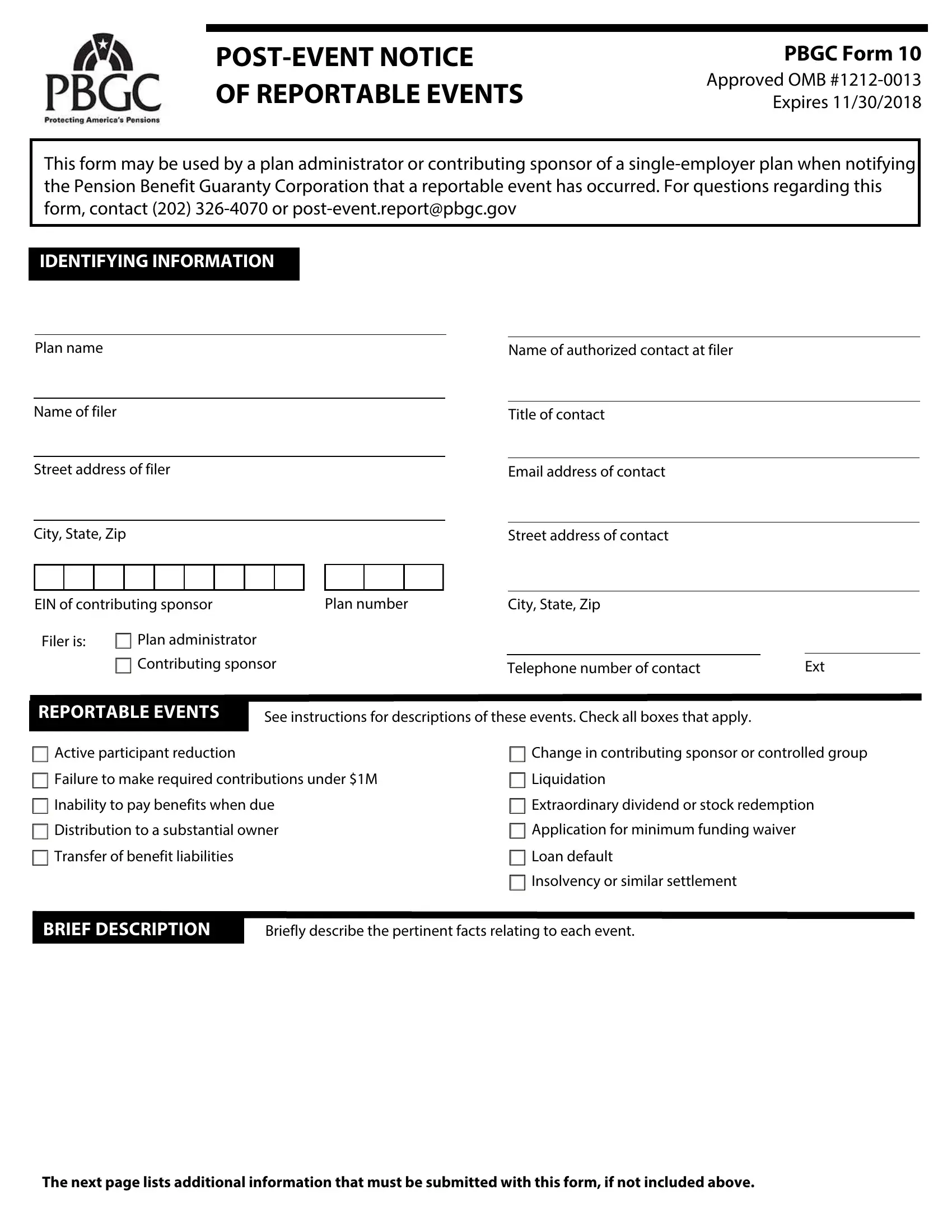
In the complex landscape of pension regulation and oversight, the Pension Benefit Guaranty Corporation (PBGC) plays a critical role in ensuring the financial security of single-employer pension plans through mechanisms like the Form 10. This form, officially known as the "POST-EVENT NOTICE OF REPORTABLE EVENTS," serves as a tool for plan administrators or contributing sponsors to notify the PBGC about certain events that could signal financial instability or changes potentially affecting the sustainability of a pension plan. Events requiring notification include, but are not limited to, significant reductions in active participants, changes in the contributing sponsor or controlled group, failures to make required contributions, liquidation events, and situations of insolvency. Additionally, the form requests detailed information about the event, such as descriptions, numbers of participants affected, financial and actuarial data, and any subsequent actions taken by the plan's administrators. The PBGC Form 10, bearing the OMB approval number 1212-0013 and with an expiration date of November 30, 2018, embodies a comprehensive reporting requirement aimed at promoting transparency and early intervention possibilities for the PBGC, thereby helping to safeguard the retirement incomes of millions of Americans.
| Question | Answer |
|---|---|
| Form Name | Form 10 Notice |
| Form Length | 4 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 1 min |
| Other names | pension form reportable, pbgc form 10 advance, pbgc form 10 search, pension form 10 pdf |
OF REPORTABLE EVENTS
PBGC Form 10
Approved OMB
This form may be used by a plan administrator or contributing sponsor of a
IDENTIFYING INFORMATION
Plan name
Name of filer
Street address of filer
City, State, Zip
EIN of contributing sponsor |
Plan number |
|
Filer is: |
Plan administrator |
|
|
Contributing sponsor |
|
Name of authorized contact at filer
Title of contact
Email address of contact
Street address of contact
City, State, Zip
Telephone number of contact |
Ext |
REPORTABLE EVENTS
See instructions for descriptions of these events. Check all boxes that apply.
Active participant reduction |
Change in contributing sponsor or controlled group |
Failure to make required contributions under $1M |
Liquidation |
Inability to pay benefits when due |
Extraordinary dividend or stock redemption |
Distribution to a substantial owner |
Application for minimum funding waiver |
Transfer of benefit liabilities |
Loan default |
|
Insolvency or similar settlement |
BRIEF DESCRIPTION
Briefly describe the pertinent facts relating to each event.
The next page lists additional information that must be submitted with this form, if not included above.
ADDITIONAL INFORMATION TO BE FILED
PBGC Form 10
Check box to indicate the item is attached. If not attached, explain on next page.
Active Participant Reduction
Single cause event - statement explaining the cause of the reduction (e.g., facility shutdown or sale, discontinued operations, winding down of the company, or reduction in force).
Attrition event - statement of factors involved in the attrition such as frozen plan, aging workforce or improved operational efficiencies that do not require replacing departing active participants
Number of active participants at the date the event occurs and at the beginning of the plan year in which the event occurred. If reporting
Failure to Make Required Contributions
Due date and amount of the missed contribution
Due date and amount of the next payment due
Due date and amount of all contributions not timely made and not reported on the last Schedule SB filed
Date and amount of any contribution(s) made related to the missed contribution(s)
Reason contribution was not made by due date
Description of the plan's controlled group structure, including the name of each controlled group member
Name of each plan maintained by any member of the plan’s controlled group, its contributing sponsor(s) and
EIN/PN
Actuarial Information (see instructions)
Financial Information (see instructions)
Inability to Pay Benefits When Due
Date of any missed benefit payment and amount of benefits due
Next date on which the plan is expected to be unable to pay benefits, the amount of the projected shortfall, and the number of plan participants expected to be affected
Amount of the plan’s liquid assets at the end of the quarter, and the amount of its disbursements for the quarter
Name, address and phone number of plan trustee (and of any custodian)
Most recent pension plan document(s)
The Internal Revenue Service Determination Letter indicating the plan is a covered plan, if applicable
Description of the plan’s controlled group structure, including the name of each controlled group member
Actuarial Information (see instructions)
Financial Information (see instructions)
Distribution to a Substantial Owner
Name, address and phone number of person receiving the distribution(s)
Amount, form and date of each distribution
Reason for distribution
Transfer of Benefit Liabilities
Name, contributing sponsor, EIN/PN, and contact information of transferee plan(s)
Description of the transferor and transferee's controlled group structures, including the name of each controlled group member
Explanation of the actuarial assumptions used in determining the value of benefit liabilities (and, if appropriate, plan assets) transferred
Estimate of the assets, liabilities, and number of participants whose benefits are transferred (liabilities and participants should be broken down by status - active, term vested, and retirees)
Financial Information for the transferor and transferee's controlled group (see instructions)
Change in Contributing Sponsor or Controlled Group
Description of the plan’s old and new controlled group structures, including the name of each controlled group member
Name of each plan maintained by any member of the plan's old and new controlled groups, its contributing sponsor(s) and EIN/PN
Financial Information for the old and new controlled group (see instructions)
Liquidation
Description of the plan's controlled group structure before and after the liquidation, including the name of each controlled group member
Operational status of each controlled group member (in Chapter 7 proceedings, liquidating outside of bankruptcy,
Name of each plan maintained by any member of the plan's controlled group, its contributing sponsor(s) and
EIN/PN
Statement whether the recipient was a member of the plan’s controlled group
Actuarial Information (see instructions)
Financial Information (see instructions)
If the plan sponsor is expected to cease or has ceased substantially all operations also provide:
•Date on which substantially all operations are expected to cease or have ceased
•Most recent pension plan document(s)
•Address of each controlled group member
•The Internal Revenue Service Determination Letter indicating the plan is a covered plan, if applicable
Extraordinary Dividend or Stock Redemption
Name and EIN of person making the distribution
Date and amount of cash distribution(s) during fiscal year
Description, fair market value, and date or dates of any
Statement whether the recipient was a member of the plan's controlled group
Financial Information (see instructions)
Application for Minimum Funding Waiver
Copy of waiver application, with all attachments
Minimum funding projections for the next 5 years (with and without the waiver) including all details supporting the calculations and all assumptions, to the extent not included in the waiver application
PBGC Form 10
Loan Default
Copy of the relevant loan documents (e.g., promissory note, security agreement, loan agreement amendments and waivers)
Due date and amount of any missed payment
Copy of any written notice of default or any notice of acceleration from lender, any notice of forbearance, or loan agreement amendment or waiver
Description of any
Description of the plan's controlled group structure, including the name of each controlled group member
Actuarial Information (see instructions)
Financial Information (see instructions)
Insolvency or Similar Settlement
Name, address and phone number of any trustee, receiver or similar person
Docket number of court filing and location of the court where any relevant proceeding was or will be filed (if known)
Description of the plan’s controlled group structure, including the name of each controlled group member
Name of each plan maintained by any member of the plan’s controlled group, its contributing sponsor(s) and
EIN/PN
Actuarial Information (see instructions)
Financial Information (see instructions)
MISSING INFORMATION
If required information has not been submitted with this Form 10, explain below.
FILING INFORMATION
Date of Event |
Notice Due Date |
Notice Filing Date (if late, explain below)
REASON FOR LATE FILING OR ATTRITION EVENT EXTENTION CLAIMED
PBGC Form 10
If filing is late or an extension for an attrition event is claimed, explain below.
CERTIFICATION
I certify that, to the best of my knowledge and belief, the information submitted in this filing is true, correct, and complete. In making this certification, I recognize that knowingly and willfully making false, fictitious, or fraudulent statements to the PBGC is punishable under 18 U.S.C. § 1001.
Signature of Individual Submitting Form |
Name and Title of Individual Submitting Form |
|
|
|
|
Telephone Number of Individual Submitting Form |
Employer of Individual Submitting Form |
|