
You'll be able to prepare 1147 form hawaii without difficulty with the help of our online tool for PDF editing. In order to make our editor better and easier to work with, we continuously design new features, bearing in mind suggestions from our users. It just takes a few simple steps:
Step 1: First, open the tool by clicking the "Get Form Button" in the top section of this site.
Step 2: Using our handy PDF editing tool, you can accomplish more than merely complete blanks. Express yourself and make your forms seem great with customized textual content put in, or modify the original content to perfection - all comes along with the capability to incorporate your personal photos and sign the PDF off.
This PDF doc will need specific information; to ensure accuracy, remember to heed the next tips:
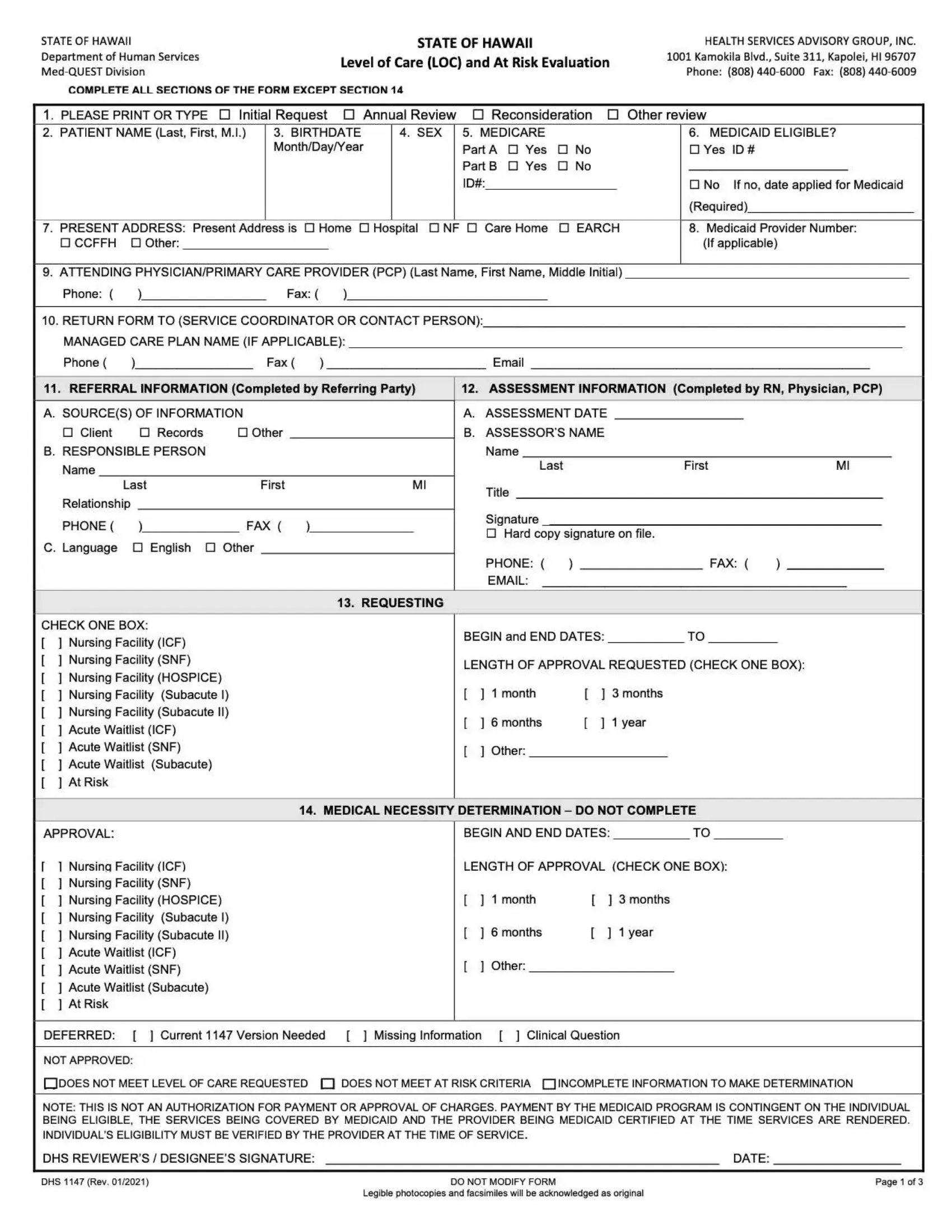
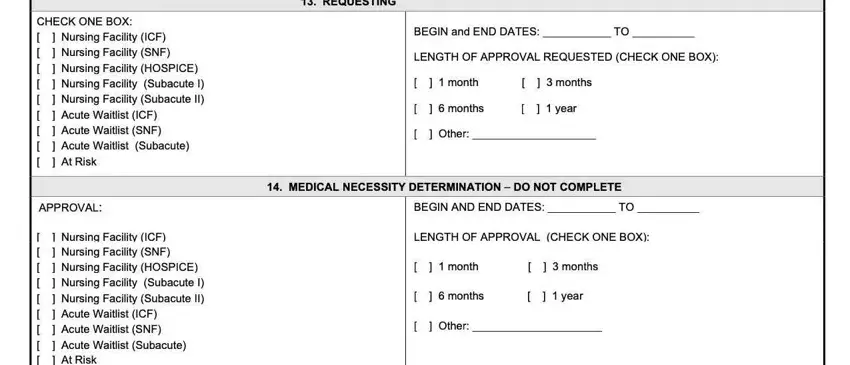
1. Fill out the 1147 form hawaii with a group of necessary fields. Note all the required information and make sure there is nothing left out!
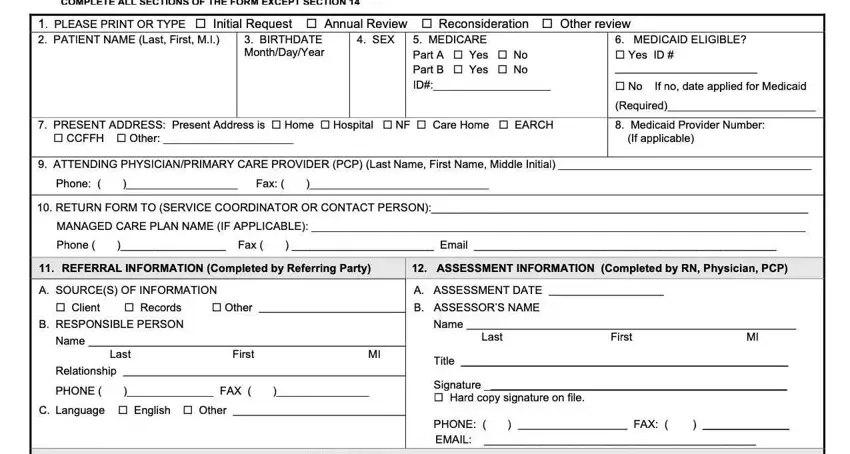
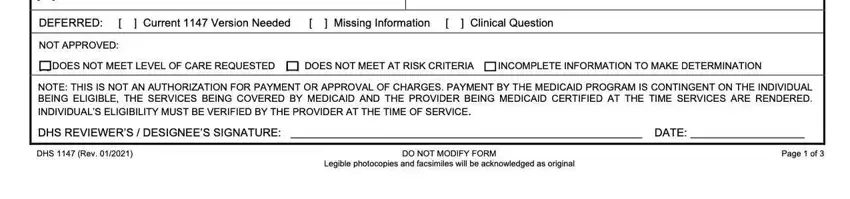
2. Your next stage would be to fill out these blanks: .
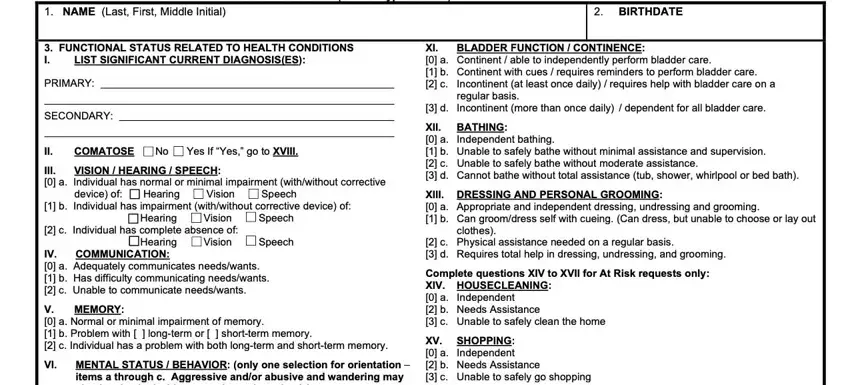
3. The third step is going to be straightforward - fill out all the fields in in order to finish the current step.
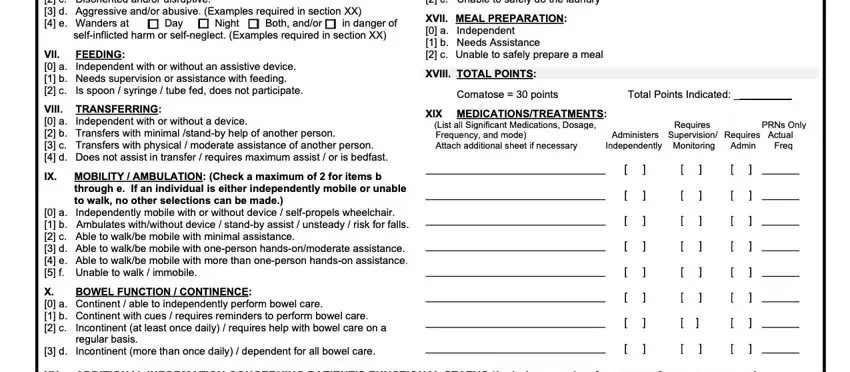
4. This fourth part arrives with all of the following empty form fields to fill out: .
People generally make some mistakes while filling out this field in this area. Ensure that you revise everything you type in right here.
5. The form should be wrapped up by filling in this area. Here one can find a full list of fields that must be completed with specific information to allow your document usage to be complete: .
Step 3: Just after double-checking the filled out blanks, press "Done" and you're good to go! Make a free trial subscription at FormsPal and acquire immediate access to 1147 form hawaii - download, email, or edit in your personal cabinet. Here at FormsPal, we endeavor to be certain that all of your details are stored secure.