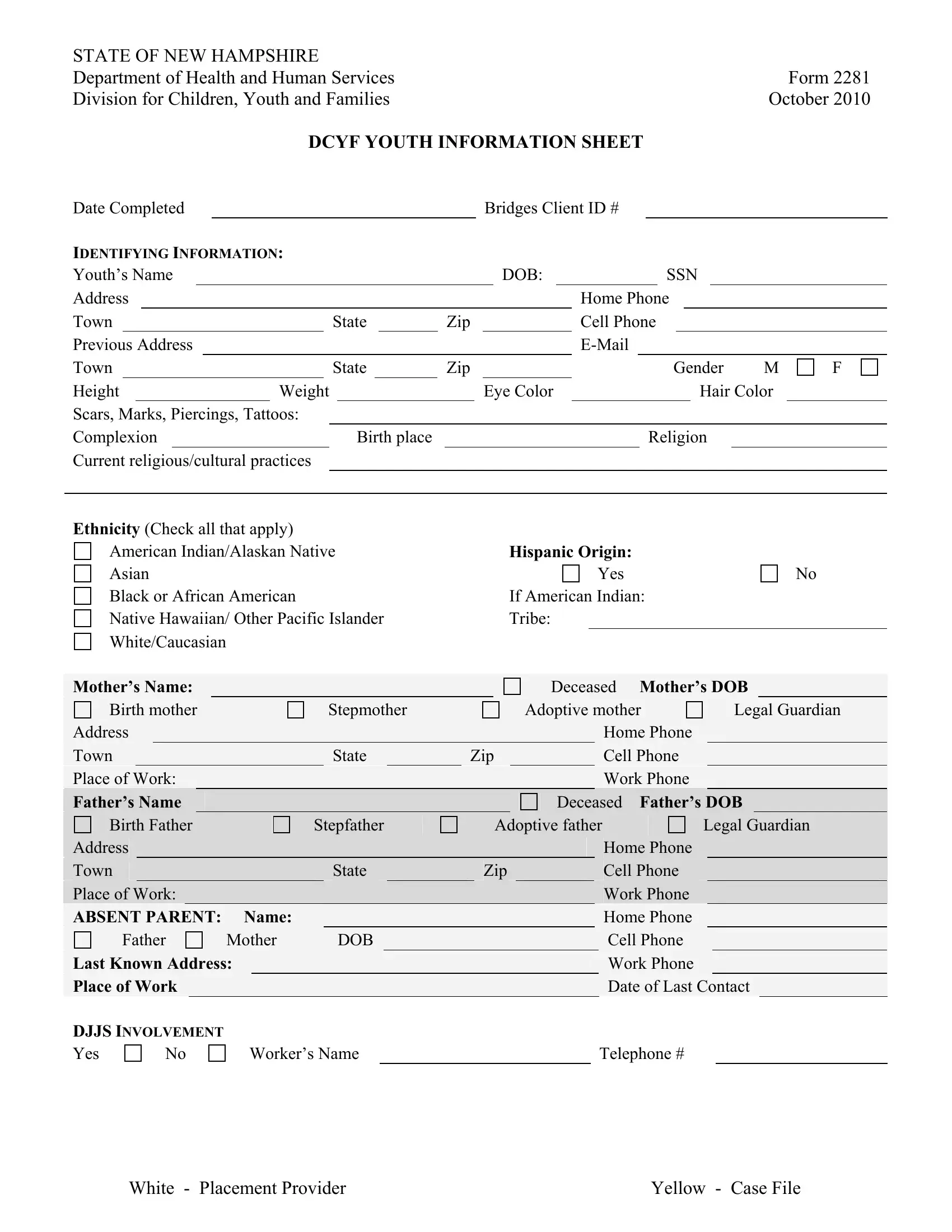
Are you familiar with IRS Form 2281? If not, you should be. This form is used by the IRS to document that a qualified employee has been transferred to work in a foreign country as part of their employment duties. The transfer must meet certain requirements in order for the employee to qualify for the foreign earned income exclusion and/or housing exclusion or deduction. Let's take a closer look at what these requirements are and how you can file Form 2281 if your situation meets them.
| Question | Answer |
|---|---|
| Form Name | Form 2281 |
| Form Length | 7 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 1 min 45 sec |
| Other names | E-Mail, 2010, DJJS, blank information template |
STATE OF NEW HAMPSHIRE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
Department of Health and Human Services |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Form 2281 |
|||||||||||||
Division for Children, Youth and Families |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
October 2010 |
||||||||||||||
|
|
|
|
|
|
|
|
DCYF YOUTH INFORMATION SHEET |
|
|
||||||||||||||||||||
Date Completed |
|
|
|
|
|
|
|
|
|
|
Bridges Client ID # |
|
|
|
||||||||||||||||
IDENTIFYING INFORMATION: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
Youth’s Name |
|
|
|
|
|
|
|
|
|
|
|
|
DOB: |
|
|
|
|
|
SSN |
|
|
|
||||||||
Address |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Home Phone |
|
|
|
||||||||||||
Town |
|
|
|
|
State |
|
|
Zip |
|
|
|
|
Cell Phone |
|
|
|
||||||||||||||
Previous Address |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
Town |
|
|
|
|
State |
|
|
Zip |
|
|
|
|
|
|
|
|
Gender |
M |
F |
|||||||||||
Height |
|
|
Weight |
|
|
|
|
Eye Color |
|
|
|
|
|
|
|
|
Hair Color |
|
||||||||||||
Scars, Marks, Piercings, Tattoos: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
Complexion |
|
|
|
|
|
Birth place |
|
|
|
|
|
|
|
|
|
Religion |
|
|
||||||||||||
Current religious/cultural practices |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Ethnicity (Check all that apply) |
|
American Indian/Alaskan Native |
Hispanic Origin: |
Asian |
Yes |
Black or African American |
If American Indian: |
Native Hawaiian/ Other Pacific Islander |
Tribe: |
White/Caucasian |
|
No
|
|
Mother’s Name: |
|
|
|
|
|
|
|
|
|
|
|
|
|
Deceased |
Mother’s DOB |
|
|
|
|||||||||||||
|
|
Birth mother |
|
|
|
|
Stepmother |
|
|
|
|
Adoptive mother |
|
|
Legal Guardian |
||||||||||||||||||
|
|
Address |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Home Phone |
|
|
|
|
|
|
|||
|
|
Town |
|
|
|
|
|
|
|
|
|
|
|
State |
|
|
|
Zip |
|
|
|
|
Cell Phone |
|
|
|
|
|
|
||||
|
|
Place of Work: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Work Phone |
|
|
|
|
|
|
||||||
|
|
Father’s Name |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Deceased |
Father’s DOB |
|
|
|
|||||||||||
|
|
Birth Father |
|
|
|
Stepfather |
|
|
|
Adoptive father |
|
|
|
Legal Guardian |
|||||||||||||||||||
|
|
Address |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Home Phone |
|
|
|
|
|
|
||
|
|
Town |
|
|
|
|
|
|
|
|
|
|
|
State |
|
|
|
Zip |
|
|
|
|
Cell Phone |
|
|
|
|
|
|
||||
|
|
Place of Work: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Work Phone |
|
|
|
|
|
|
||||
|
|
ABSENT PARENT: |
|
Name: |
|
|
|
|
|
|
|
|
|
|
|
|
Home Phone |
|
|
|
|
|
|
||||||||||
|
|
Father |
|
|
|
|
Mother |
|
DOB |
|
|
|
|
|
|
|
|
|
|
Cell Phone |
|
|
|
|
|
|
|||||||
|
|
Last Known Address: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Work Phone |
|
|
|
|
|
|
|||||||||
|
|
Place of Work |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Date of Last Contact |
|
|
||||||||
DJJS INVOLVEMENT
Yes
No
Worker’s Name |
|
Telephone # |
White - Placement Provider |
Yellow - Case File |
Additional Adults in household |
|
Relationship |
(Add additional names to the back of page) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Names of Siblings (in or out of the |
If other |
|
DOB |
|||
(in the home) (Add additional names to the back of page) |
checked, |
|
|
|||
|
|
|
|
please |
|
|
|
|
|
|
specify |
|
|
|
Sibling |
Other |
|
|
|
|
|
Sibling |
Other |
|
|
|
|
|
Sibling |
Other |
|
|
|
|
|
Sibling |
Other |
|
|
|
|
|
Sibling |
Other |
|
|
|
|
|
Sibling |
Other |
|
|
|
|
In Household
Yes No
Yes No
Yes No
Yes No
Yes No
Yes No
|
EDUCATION & SCHOOL |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
SAU# |
|
|
|
|
|
|
|
|
|
|
|
Home Schooled |
|
|
|
|
|
|
|||||
|
Current School: |
|
|
|
|
|
|
|
|
|
Current Grade: |
|
|
|
|
|
|
|
|
|
|
|||
|
Last School Attended: |
|
|
|
|
|
|
|
|
Last Grade Completed: |
|
|
|
|
|
|
|
|||||||
|
Current School Telephone |
|
|
|
|
|
|
Receive Special Education |
|
|
|
|
|
Yes |
|
No |
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
504 Plan |
|
Yes |
|
|
No |
Latest IEP Date: |
|
|
|
|
Educational Coding |
|
|
|
|
||||||||
|
Educational Surrogate |
|
|
|
|
|
Surrogate’s phone # |
|
|
|
|
|
|
|
|
|
||||||||
|
Have friends at school? |
|
Yes |
No |
|
|
Know how to read? |
|
|
|
Yes |
|
No |
|
||||||||||
|
Like the teachers? |
|
|
|
|
Yes |
No |
|
|
Know how to write: |
|
|
|
Yes |
|
No |
|
|||||||
|
Like school? |
|
|
|
|
Yes |
No |
|
|
Sports/School activities? |
|
|
|
Yes |
|
No |
|
|||||||
|
Resist going to school? |
|
Yes |
No |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
School |
Behaviorally |
Poor |
Fair |
Good |
Great |
Excellent |
|
Performance |
Academically |
Poor |
Fair |
Good |
Great |
Excellent |
|
Has youth ever been expelled or suspended? |
Yes |
No |
If “yes”, explain |
|
|||
|
|
|
|
|
|
|
|
EMPLOYMENT OR VOLUNTEER WORK. |
|
|
|
|
|
|
|
|
|||
Currently Employed |
Yes |
No |
If Yes: Employer Name: |
|
|
|
|
||||
Address |
|
|
|
|
|
|
Work Phone number: |
|
|
||
Average Hours Worked Per Week: |
|
|
|
Interested in getting a job? |
|
Yes |
No |
||||
Perform community service or volunteer work? |
|
Yes |
No |
If Yes please describe: |
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
White - Placement Provider |
Yellow - Case File |
BIRTH FAMILY HISTORY (check all that apply) |
|
|
Please specify type next to: ** |
Mother |
Father |
Allergies** Cancer** Mental Illness** Substance Abuse** Epilepsy (other seizure disorder)** Neurological Disorder** Tuberculosis Diabetes Suicidal Kidney Disease Heart Disease Others** Comments:
PHYSICAL & MENTAL HEALTH
Name of Youth’s Primary Care Physician |
|
|
|
|
|
|
Last Physical Exam |
|
|
||||||||||
Address: |
|
|
|
|
|
|
|
|
|
|
Office Phone |
|
|
|
|
|
|||
Insurance Carrier: |
|
|
|
|
|
|
ID No. |
|
|
|
|
Medicaid No. |
|
|
|
||||
Allergies to medication (specify): |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
Allergies to food (specify): |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
Other Allergies (specify): |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Current Medications: |
|
Prescribed by: |
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
Taken: |
AM |
PM |
Both |
In School |
|||||
|
|
|
|
|
|
|
|
|
|
Taken: |
AM |
PM |
Both |
In School |
|||||
|
|
|
|
|
|
|
|
|
|
Taken: |
AM |
PM |
Both |
In School |
|||||
|
|
|
|
|
|
|
|
|
|
Taken: |
AM |
PM |
Both |
In School |
|||||
|
|
|
|
|
|
|
|
|
|
Taken: |
AM |
PM |
Both |
In School |
|||||
|
|
|
|
|
|
|
|
|
|
Taken: |
AM |
PM |
Both |
In School |
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Name of Therapist /Psychiatrist |
|
|
|
|
|
|
|
|
|
|||
Address |
|
|
|
|
|
|
|
|
Office Phone |
|
|
|
Frequency of visits: |
|
|
|
|
|
|
Last session |
|
|
|||
Name of Dentist: |
|
|
|
Last Dental Exam: |
|
|
|
|||||
Address |
|
|
|
|
|
|
|
|
Office Phone |
|
|
|
Does youth wear eyeglasses? |
Yes |
No |
Contact lenses? |
Yes |
No |
|||||||
Name of Eye Doctor: |
|
|
|
|
|
Last Vision Exam: |
|
|
||||
Other Physicians: |
|
|
|
|
|
|
|
|
|
|
|
|
Medical and Psychiatric Hospitalizations (dates & locations)
White - Placement Provider |
Yellow - Case File |
Diagnosed Medical and Psychiatric Conditions:
Tobacco Use: |
Yes |
|
No |
Prior or Current Drug Treatment |
Yes |
No |
If YES, where |
|||||
and when |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Drug Use: |
Yes |
|
No |
|
|
If yes: |
Marijuana |
|
|
LSD |
||
Opiates |
Steroids |
|
Amphetamines |
|
Cocaine |
|
|
Ecstasy |
||||
Methamphetamine |
|
|
|
Benzodiazepines |
|
|||||||
Other |
|
|
|
|
|
|
|
|
|
|
|
|
Alcohol Use |
|
Yes |
|
No |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
SPEECH, HEARING & LANGUAGE. |
|
|
|
|
|
|
|
|
|
|||
Primary language spoken in the home: |
|
|
|
|
|
|
|
|
||||
Speaks more than one Language? |
|
Yes |
No |
|
Speech impairment? |
Yes |
No |
|||||
Hearing impairment? |
|
|
|
Yes |
No |
|
American Sign Language |
Reads |
Signs |
|||
Interpreter Needed? |
|
|
|
Yes |
No |
|
If yes, what language? |
|
|
|
||
CHILDHOOD DISEASE HISTORY (Check all that apply)
Bronchitis |
Chicken Pox |
Ear Infections |
|
German Measles |
Heart Disease |
Measles |
|
Pneumonia |
Tuberculosis |
Other (please specify) |
|
Immunization History Received |
|
Yes |
No |
Epilepsy or other seizure disorder Mumps
DIET & NUTRITION FOR YOUTH. |
|
|
|
|
|
Diagnosed eating disorders? |
Yes |
No |
Require a special diet? |
Yes |
No |
If Yes to either question please specify: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
SLEEPING PATTERN: |
|
|
|
|
|
|
|
|
|
Usual Bedtime |
|
|
|
|
|
Usual wake time |
|
|
|
Please describe sleeping pattern |
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|||
Any diagnosed sleep disorders |
|
Yes |
No |
|
|
||||
If yes, please explain |
|
|
|
|
|
|
|
|
|
Bed Wetting |
Yes |
No |
Nightmares |
Yes |
No |
||||
White - Placement Provider |
Yellow - Case File |
STRENGTHS AND RESOURCES.
Often |
Sometimes |
Never |
Often |
Sometimes |
Never |
Benefits from structure Creative
Good
Club or group involvement Engaging personality Healthy
Skill or interest in athletics
OBSERVED BEHAVIORS. Identify the youth’s behaviors that may result in harm or injury to self or others:
Often |
Sometimes |
Never |
Often |
Sometimes |
Never |
Aggressive
Destructive
Tantrums
Poor
Details and Comments:
Assaultive
Cruel to Animals
Difficulty Concentrating
Fire setting
Lying
Stealing
Parentified
Running Away
Other:
RECREATION & LEISURE.
Does youth have a boyfriend or girlfriend? (Romantic involvement) |
Yes |
No |
|||||
Does youth participate in structured community or school extracurricular activities or events |
Yes |
No |
|||||
Details: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Is youth involved in a gang or cult? |
Yes |
No |
Describe: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
What does youth do for recreation or hobbies?
White - Placement Provider |
Yellow - Case File |

IMPORTANT PEOPLE IN THE YOUTH’S LIFE (CONNECTIONS) |
|
|
|
Name |
Address |
Telephone |
Relationship |
|
|
Number |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
This information is authorized to be shared with community based service providers, residential placement providers for the purposes of case planning and in order to maintain safety, permanency and
Signature of Parent/Guardian |
|
Date |
|
||
Signature of CPSW |
|
Date |
|
||
Name & Address of CPSW |
|
|
|
||
Signature of Placement Provider |
|
Date |
|
||
Name & Address of Placement Provider |
|
|
|
||
Signature of Foster Care Provider |
|
Date |
|
||
Name & Address of Foster Care Provider |
|
|
|
||
Form Completed by: |
|
Date |
|
||
This section to be completed by the CPSW
The GAL/Casa assigned to the youth
Telephone Number
PD
White - Placement Provider |
Yellow - Case File |
STATE OF NEW HAMPSHIRE |
Form 2281(i) |
Department of Health and Human Services |
October, 2010 |
Division for Children, Youth and Families |
|
Instructions for the Youth Information Sheet (Form 2281)
PURPOSE;
The Youth Information Sheet provides essential information about the youth to the youth’s family and providers who have responsibility for the youth’s care.
INSTRUCTIONS:
The “Youth Information Sheet” is a
The “Youth Information Sheet” must be updated every 6 months while the youth remains in placement.
The current substitute care provider retains the original “Youth Information Sheet”. A copy must be retained in the case file. The youth’s subsequent care provider must be provided with the latest version of the “Youth Information Sheet”.
FORM COMPLETION:
By signing the form, the substitute care provider or parent of the returning youth acknowledges receipt of the document.
Enter as much accurate and detailed information that identifies the youth and provides essential details about his or her physical and behavioral health, school, habits and personality. Detail specific behaviors of the youth important for the current or future caregiver to know about, such as education needs, volunteer or employment interests, running away, suicide threats or attempts, and sleepwalking and other significant behaviors or needs of the youth.
1)Enter “NA” to indicate any information that is “not available” or “not applicable”.
2)Under Observed Behaviors add specific comments about behavioral health issues.
3)Sign and enter the name of the CPSW and location of the CPSW’s office.
4)Obtain the signature of the parent, foster parent or residential care provider.
RETENTION:
The “Youth Information Sheet” is retained in the case file.
PD