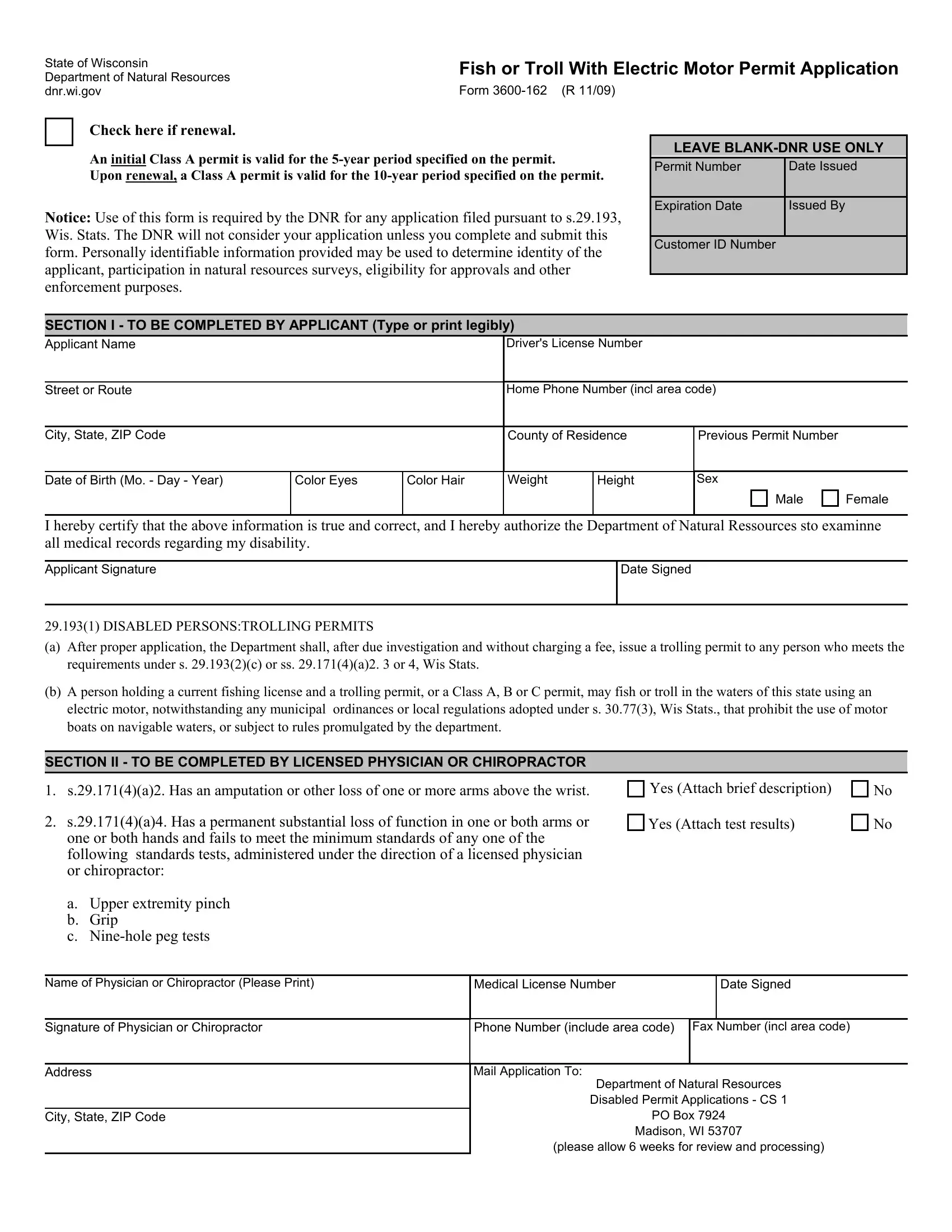
Fishing is a beloved pastime for many, offering a blend of relaxation, sport, and engagement with the natural environment. Within this context, the State of Wisconsin has established specific guidelines to ensure accessibility and inclusivity for individuals with disabilities through the Form 3600-162, a critical document for those seeking to use electric motors for fishing or trolling in state waters. Issued by the Department of Natural Resources (DNR), this permit application embodies the state’s commitment to enabling all individuals to participate in fishing activities, reflecting broader legal and environmental principles. This permit, which requires renewal, comes in the initial form of a five-year Class A permit, further extending to ten years upon renewal. It delineates a process that necessitates an applicant's detailed personal information, certification of the data’s accuracy, and authorization for the DNR to review medical records related to the applicant's disability. Moreover, the form includes provisions for a licensed physician or chiropractor to attest to the applicant's qualifying disability status, signaling a layered and thorough approach to verifying eligibility. Central to this document is not only the logistical framework it provides for applicants and the DNR but also the legal foundation it rests upon, specifically stipulations outlined in s.29.193, Wis. Stats., which guide the issuance of trolling permits to eligible individuals. Through Form 3600-162, Wisconsin encapsulates its legal and moral responsibility towards ensuring equitable fishing rights, paving the way for a more inclusive and diverse engagement with the state’s natural resources.
| Question | Answer |
|---|---|
| Form Name | Form 3600 162 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | 3600162 dnr service center application form # 3600 162 |
State of Wisconsin |
Fish or Troll With Electric Motor Permit Application |
|||||||
Department of Natural Resources |
||||||||
|
|
|
|
|
|
|||
dnr.wi.gov |
Form |
|
|
|
|
|||
|
Check here if renewal. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
An initial Class A permit is valid for the |
|
LEAVE |
|||||
|
|
|||||||
|
|
|
|
|
|
|||
|
|
Permit Number |
|
Date Issued |
|
|||
|
Upon renewal, a Class A permit is valid for the |
|
|
|||||
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
Expiration Date |
|
Issued By |
||
Notice: Use of this form is required by the DNR for any application filed pursuant to s.29.193,
Wis. Stats. The DNR will not consider your application unless you complete and submit this
form. Personally identifiable information provided may be used to determine identity of the applicant, participation in natural resources surveys, eligibility for approvals and other enforcement purposes.
SECTION I - TO BE COMPLETED BY APPLICANT (Type or print legibly)
Customer ID Number
Applicant Name |
|
|
Driver's License Number |
|
|
|
|
|
|
|
|
|
|
|
|
||||
Street or Route |
|
|
Home Phone Number (incl area code) |
|
|||||
|
|
|
|
|
|
||||
City, State, ZIP Code |
|
|
County of Residence |
Previous Permit Number |
|
||||
|
|
|
|
|
|
|
|
|
|
Date of Birth (Mo. - Day - Year) |
Color Eyes |
Color Hair |
Weight |
Height |
Sex |
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Male |
Female |
|
|
|
|
|
|
|
|
|
|
|
I hereby certify that the above information is true and correct, and I hereby authorize the Department of Natural Ressources sto examinne all medical records regarding my disability.
Applicant Signature
Date Signed
29.193(1) DISABLED PERSONS:TROLLING PERMITS
(a)After proper application, the Department shall, after due investigation and without charging a fee, issue a trolling permit to any person who meets the requirements under s. 29.193(2)(c) or ss. 29.171(4)(a)2. 3 or 4, Wis Stats.
(b)A person holding a current fishing license and a trolling permit, or a Class A, B or C permit, may fish or troll in the waters of this state using an electric motor, notwithstanding any municipal ordinances or local regulations adopted under s. 30.77(3), Wis Stats., that prohibit the use of motor boats on navigable waters, or subject to rules promulgated by the department.
SECTION II - TO BE COMPLETED BY LICENSED PHYSICIAN OR CHIROPRACTOR
1.s.29.171(4)(a)2. Has an amputation or other loss of one or more arms above the wrist.
2.s.29.171(4)(a)4. Has a permanent substantial loss of function in one or both arms or one or both hands and fails to meet the minimum standards of any one of the following standards tests, administered under the direction of a licensed physician or chiropractor:
Yes (Attach brief description)
Yes (Attach test results)
No
No
a. |
Upper extremity pinch |
|
|
|
b. |
Grip |
|
|
|
c. |
|
|
|
|
|
|
|
|
|
Name of Physician or Chiropractor (Please Print) |
Medical License Number |
|
Date Signed |
|
|
|
|
|
|
Signature of Physician or Chiropractor |
Phone Number (include area code) |
Fax Number (incl area code) |
||
|
|
|
|
|
Address |
Mail Application To: |
|
|
|
|
|
Department of Natural Resources |
||
|
|
Disabled Permit Applications - CS 1 |
||
City, State, ZIP Code |
PO Box 7924 |
|||
|
|
Madison, WI 53707 |
||
|
|
(please allow 6 weeks for review and processing) |
||