
You may complete surgery clearance form effortlessly with our PDFinity® editor. To have our editor on the cutting edge of practicality, we strive to implement user-driven capabilities and enhancements regularly. We are at all times looking for suggestions - join us in revolutionizing PDF editing. Starting is effortless! All you need to do is adhere to the next simple steps down below:
Step 1: First of all, open the editor by clicking the "Get Form Button" in the top section of this webpage.
Step 2: After you launch the editor, you'll see the document prepared to be completed. Besides filling out various blanks, you might also do other sorts of things with the form, particularly putting on your own text, modifying the original textual content, adding illustrations or photos, placing your signature to the form, and more.
This form will require you to type in some specific information; to guarantee accuracy and reliability, you need to take note of the guidelines just below:
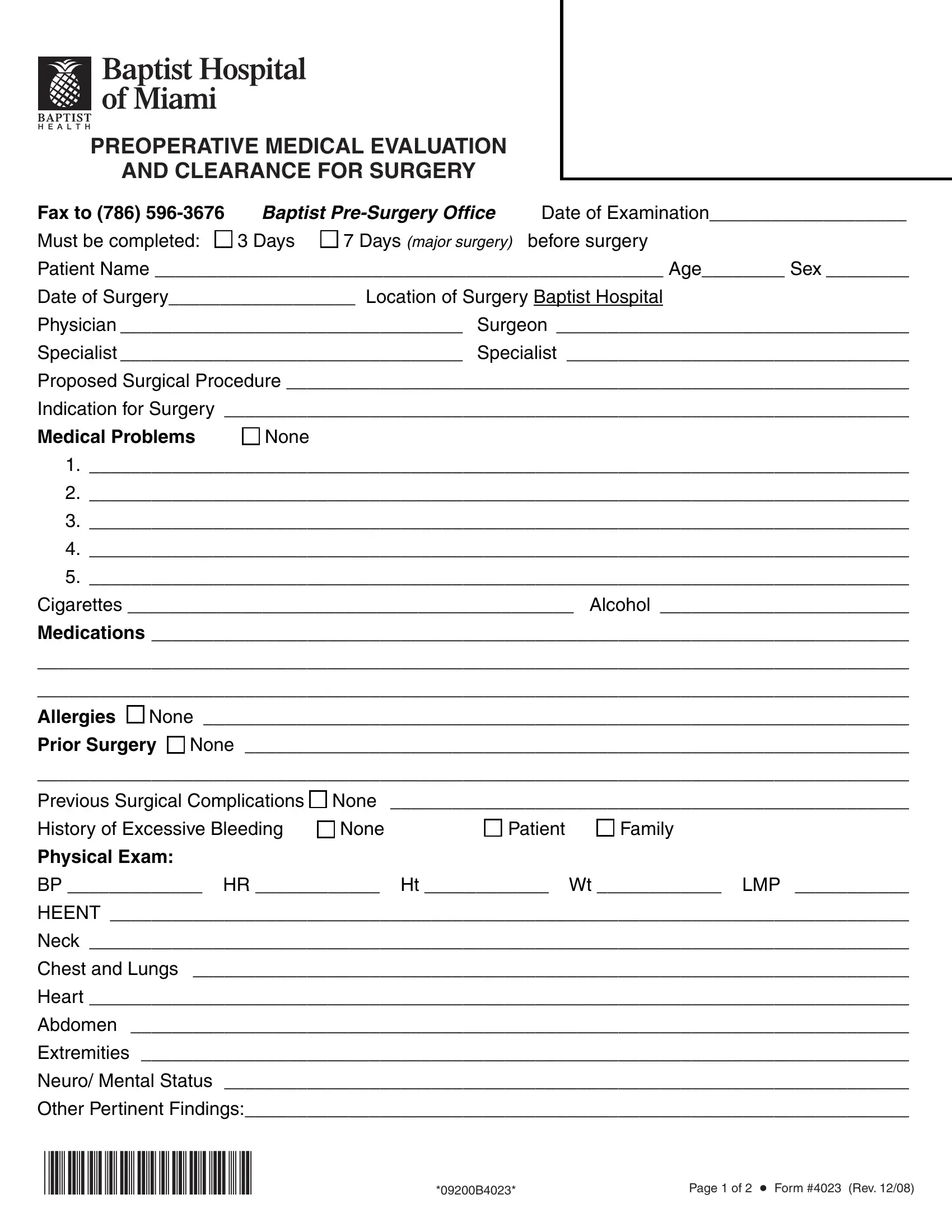
1. You need to complete the surgery clearance form properly, therefore be attentive while filling out the parts comprising these blanks:
2. After this section is done, you have to insert the required details in Medications, Allergies G None Prior Surgery G, BP HR Ht Wt LMP, HEENT, Neck, Chest and Lungs, Heart, Abdomen, Extremities, Neuro Mental Status, and Other Pertinent Findings allowing you to move on further.
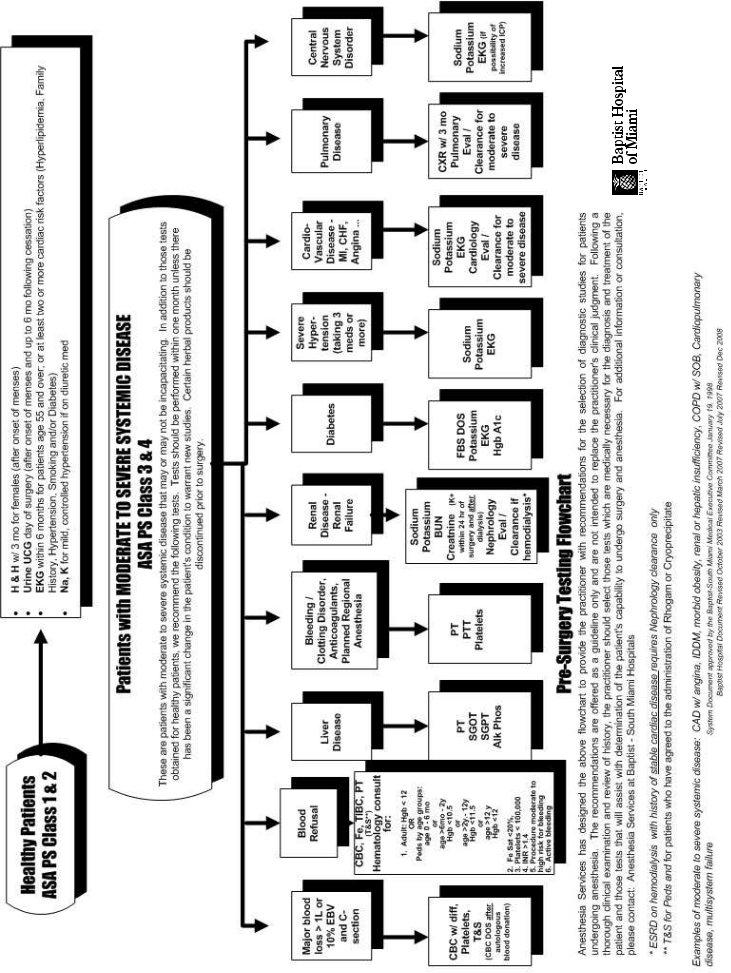
3. The next stage is normally hassle-free - fill in all the empty fields in G G G G G G G G G G, EKG, CXR, CBC, Chemistry, PTPTT, Cardiac Echo, StressCath, HgbAlC Diabetic patients, SCrCl PCN allergy, Other, Recommendations G The patient is, and G Delayed Surgery should be in order to finish this segment.
4. This particular paragraph comes with these particular empty form fields to fill out: G Delayed Surgery should be, G The patient is in optimal, Instructions to patients, Signature, MD Name, and Specialty Date.
It is easy to make an error while filling in the Specialty Date, for that reason ensure that you go through it again before you'll finalize the form.
Step 3: Look through what you've inserted in the blanks and press the "Done" button. Right after getting afree trial account with us, you will be able to download surgery clearance form or email it immediately. The PDF file will also be accessible in your personal cabinet with all of your changes. When using FormsPal, you can easily fill out documents without needing to be concerned about data incidents or entries being distributed. Our protected software ensures that your private data is kept safe.