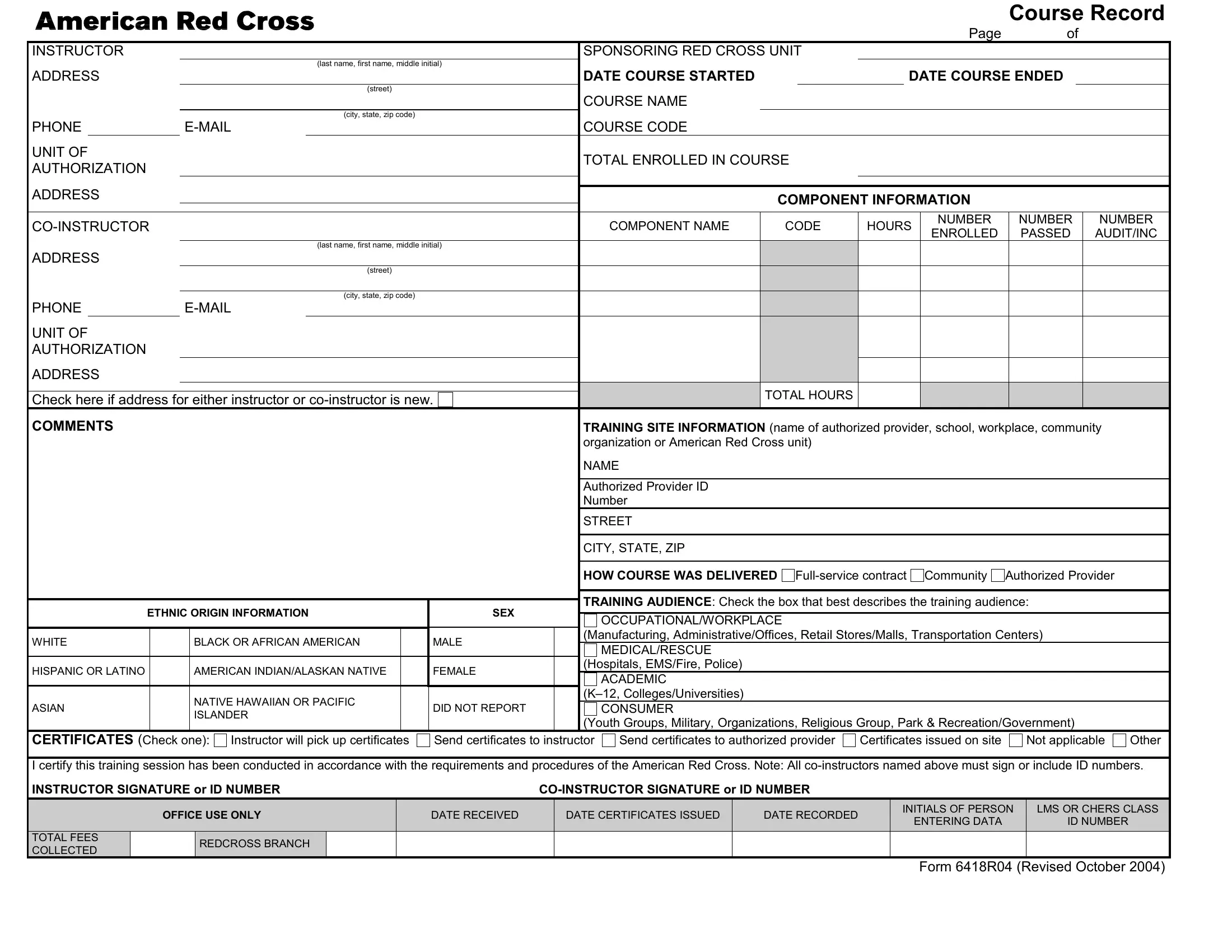
When it comes to ensuring the quality and consistency of educational courses, especially those with critical life-saving skills at their heart, the documentation and certification process is key. This is where the 6418R04 form comes into play, a crucial piece of the administrative puzzle for courses endorsed or offered by the American Red Cross. This detailed form serves several vital functions, from recording the specifics of the course such as the name, code, total hours, and the instructor and co-instructor's details, to capturing the essence of the training audience including demographics and the occupational context of the participants. Furthermore, the form lays out a structured method for noting the start and end dates of the course, enrollment numbers, and outcomes in terms of participants passed or in need of further auditing. It even accommodates details pertaining to the issuing of certificates, a fundamental aspect of course completion, allowing options for distribution mode while requiring the instructor's certification that the training was conducted as per American Red Cross standards. Beyond its functional role, the form embodies the essence of organized and responsible record-keeping, ensuring that the training delivered holds up to scrutiny and maintains the integrity the Red Cross is known for worldwide.
| Question | Answer |
|---|---|
| Form Name | Form 6418R04 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | 6418R04, E-MAIL, course record addendum form 6418ardendum, CHERS |
Course Record
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Page |
of |
|
|
|
INSTRUCTOR |
|
|
|
|
|
|
|
|
SPONSORING RED CROSS UNIT |
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
(last name, first name, middle initial) |
|
|
|
|
|
|
|
|
|
|
|
|
||||
ADDRESS |
|
|
|
|
|
|
|
|
DATE COURSE STARTED |
|
|
|
|
DATE COURSE ENDED |
|
|
||||||||
|
|
|
|
|
|
|
|
(street) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
COURSE NAME |
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
(city, state, zip code) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PHONE |
|
|
|
|
|
|
|
|
|
|
COURSE CODE |
|
|
|
|
|
|
|
|
|
||||
UNIT OF |
|
|
|
|
|
|
|
|
|
|
TOTAL ENROLLED IN COURSE |
|
|
|
|
|
|
|
||||||
AUTHORIZATION |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
ADDRESS |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
COMPONENT INFORMATION |
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
COMPONENT NAME |
CODE |
HOURS |
NUMBER |
NUMBER |
NUMBER |
|
||||||||||
|
|
|
|
|
|
|
ENROLLED |
PASSED |
AUDIT/INC |
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
(last name, first name, middle initial) |
|
|
|
|
|
|
|
|
|
|||||||
ADDRESS |
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
(street) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
(city, state, zip code) |
|
|
|
|
|
|
|
|
|
|
|
|
||||
PHONE |
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
UNIT OF |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
AUTHORIZATION |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
ADDRESS |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
TOTAL HOURS |
|
|
|
|
|
|
|||
Check here if address for either instructor or |
|
|
|
|
|
|
||||||||||||||||||
COMMENTS |
|
|
|
|
|
|
|
|
|
|
TRAINING SITE INFORMATION (name of authorized provider, school, workplace, community |
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
organization or American Red Cross unit) |
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
NAME |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Authorized Provider ID |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Number |
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
STREET |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CITY, STATE, ZIP |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
HOW COURSE WAS DELIVERED |
|
Community |
Authorized Provider |
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
TRAINING AUDIENCE: Check the box that best describes the training audience: |
|
|
||||||||
|
|
ETHNIC ORIGIN INFORMATION |
|
|
|
|
SEX |
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
OCCUPATIONAL/WORKPLACE |
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
WHITE |
|
|
|
|
BLACK OR AFRICAN AMERICAN |
|
MALE |
|
(Manufacturing, Administrative/Offices, Retail Stores/Malls, Transportation Centers) |
|
|
|||||||||||||
|
|
MEDICAL/RESCUE |
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
HISPANIC OR LATINO |
|
|
|
AMERICAN INDIAN/ALASKAN NATIVE |
|
FEMALE |
|
(Hospitals, EMS/Fire, Police) |
|
|
|
|
|
|
|
|
|
|
||||||
|
|
ACADEMIC |
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
NATIVE HAWAIIAN OR PACIFIC |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
ASIAN |
|
|
|
|
|
DID NOT REPORT |
|
CONSUMER |
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
ISLANDER |
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
(Youth Groups, Military, Organizations, Religious Group, Park & Recreation/Government) |
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
CERTIFICATES (Check one): Instructor will pick up certificates Send certificates to instructor Send certificates to authorized provider Certificates issued on site Not applicable Other
I certify this training session has been conducted in accordance with the requirements and procedures of the American Red Cross. Note: All
INSTRUCTOR SIGNATURE or ID NUMBER |
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
OFFICE USE ONLY |
|
|
DATE RECEIVED |
|
DATE CERTIFICATES ISSUED |
DATE RECORDED |
|
INITIALS OF PERSON |
LMS OR CHERS CLASS |
|
|
|
|
|
|
|
|
ENTERING DATA |
ID NUMBER |
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
||
TOTAL FEES |
|
|
REDCROSS BRANCH |
|
|
|
|
|
|
|
|
|
|
COLLECTED |
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Form 6418R04 (Revised October 2004)