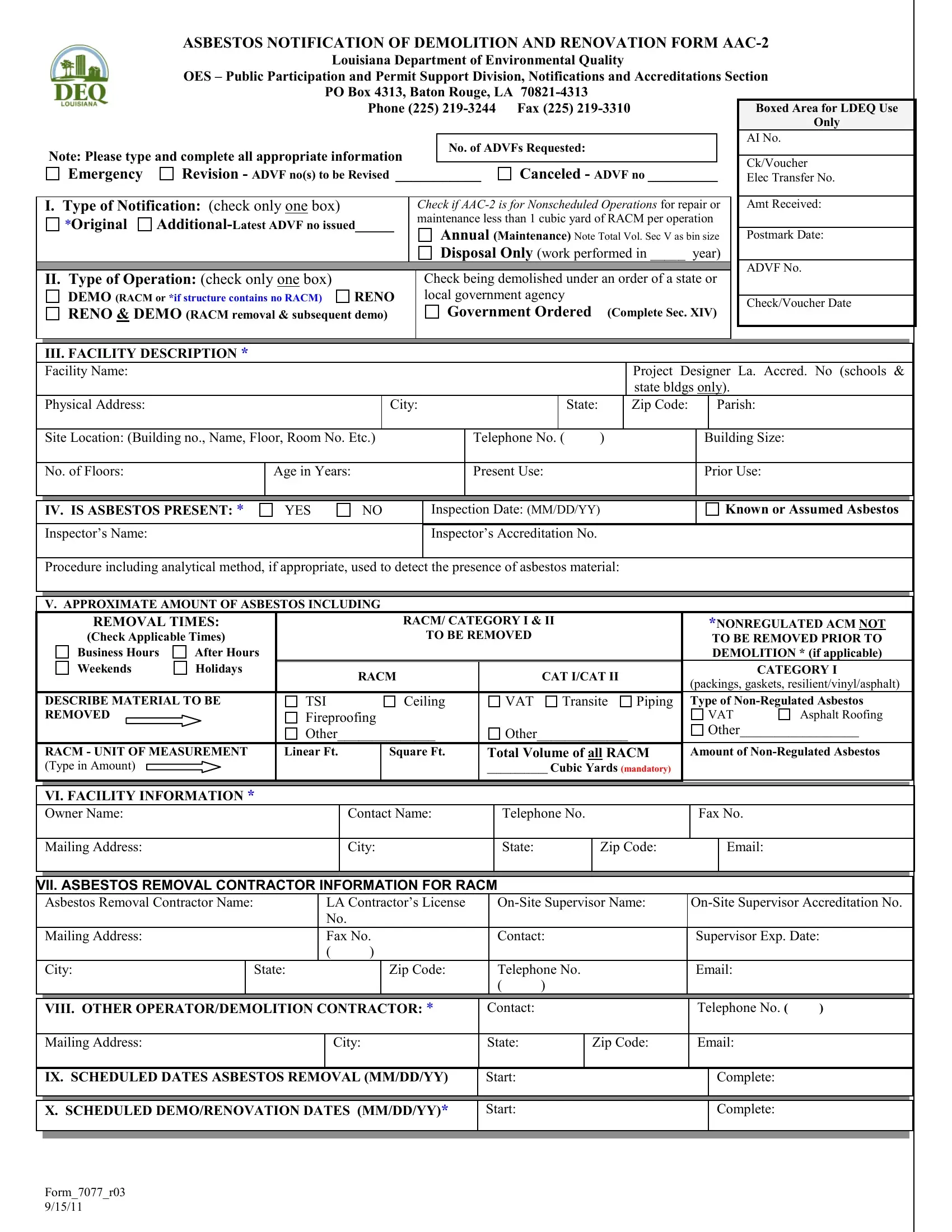
Managing asbestos during demolition and renovation projects requires meticulous planning and strict compliance with environmental regulations. This is where the 7077 R03 form, titled "Asbestos Notification of Demolition and Renovation Form," plays a crucial role. Issued by the Louisiana Department of Environmental Quality, specifically the Public Participation and Permit Support Division, Notifications and Accreditations Section, this document is essential for contractors and property owners intending to undertake construction work that might involve asbestos. The form serves multiple purposes: it alerts the department about the potential disturbance of asbestos-containing materials, outlines the scope of the demolition or renovation activity, and details the methods for asbestos management and disposal. To complete the form, one must provide a comprehensive facility description, confirm the presence or absence of asbestos through an inspection, and describe the planned procedures for handling and disposing of asbestos material. The form also necessitates information about the removal contractor, solid waste transporter, and the disposal site for the asbestos waste. Moreover, it includes sections for emergency renovations involving asbestos and a declaration for projects where no regulated asbestos-containing material is found. With options for indicating emergency situations and government-ordered demolitions, the form underscores the varied scenarios that might necessitate its use. It culminates with a certification that all provided information is accurate and that all activities will comply with local regulations, emphasizing the legal responsibilities of the parties involved.
| Question | Answer |
|---|---|
| Form Name | Form 7077 R03 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | form aac 2 printable, form aac 2 print, louisiana notification demolition printable, louisiana aac 2 form |
ASBESTOS NOTIFICATION OF DEMOLITION AND RENOVATION FORM
|
|
|
|
|
Louisiana Department of Environmental Quality |
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
OES – Public Participation and Permit Support Division, Notifications and Accreditations Section |
|
|
||||||||||||||||||||||||
|
|
|
|
|
PO Box 4313, Baton Rouge, LA |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
Phone (225) |
|
|
|
|
|
|
|
|
Boxed Area for LDEQ Use |
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Only |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
AI No. |
|
|
|
Note: Please type and complete all appropriate information |
|
|
|
|
No. of ADVFs Requested: |
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Ck/Voucher |
|
|
|||||||
|
Emergency |
|
Revision - ADVF no(s) to be Revised ___________ |
Canceled - ADVF no _________ |
|
|
|
||||||||||||||||||||||
|
|
|
Elec Transfer No. |
|
|
||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
I. Type of Notification: (check only one box) |
|
|
|
|
Check if |
|
|
Amt Received: |
|
|
||||||||||||||||||
|
*Original |
|
|
maintenance less than 1 cubic yard of RACM per operation |
|
|
|
|
|
||||||||||||||||||||
|
|
|
|
|
Annual (Maintenance) Note Total Vol. Sec V as bin size |
|
|
Postmark Date: |
|
|
|||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
Disposal Only (work performed in _____ |
year) |
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
ADVF No. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
II. Type of Operation: (check only one box) |
|
|
|
|
|
Check being demolished under an order of a state or |
|
|
|
|
|
|||||||||||||||||
|
DEMO (RACM or *if structure contains no RACM) |
RENO |
|
|
|
local government agency |
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Check/Voucher Date |
|
|
|||||||||||||
|
RENO & DEMO (RACM removal & subsequent demo) |
|
|
|
|
Government Ordered |
(Complete Sec. XIV) |
|
|
|
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
III. FACILITY DESCRIPTION * |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
Facility Name: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Project Designer La. Accred. No (schools & |
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
state bldgs only). |
|
|
|
|
||||||
|
Physical Address: |
|
|
|
|
|
City: |
|
State: |
|
|
Zip Code: |
|
|
|
Parish: |
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
Site Location: (Building no., Name, Floor, Room No. Etc.) |
|
|
|
|
|
Telephone No. ( |
) |
|
|
|
|
Building Size: |
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
No. of Floors: |
|
|
Age in Years: |
|
|
|
|
|
|
|
Present Use: |
|
|
|
|
|
|
Prior Use: |
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
IV. IS ASBESTOS PRESENT: * |
|
YES |
NO |
|
|
|
Inspection Date: (MM/DD/YY) |
|
|
|
|
|
Known or Assumed Asbestos |
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
Inspector’s Name: |
|
|
|
|
|
|
|
|
|
Inspector’s Accreditation No. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
Procedure including analytical method, if appropriate, used to detect the presence of asbestos material: |
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
V. APPROXIMATE AMOUNT OF ASBESTOS INCLUDING |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
REMOVAL TIMES: |
|
|
|
|
RACM/ CATEGORY I & II |
|
|
|
|
|
|
|
*NONREGULATED ACM NOT |
|
|
|||||||||||||
|
(Check Applicable Times) |
|
|
|
|
|
|
|
TO BE REMOVED |
|
|
|
|
|
|
|
TO BE REMOVED PRIOR TO |
|
|
||||||||||
|
Business Hours |
After Hours |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DEMOLITION * (if applicable) |
|
|
|||||
|
Weekends |
|
Holidays |
|
|
RACM |
|
|
|
|
|
|
|
CAT I/CAT II |
|
|
|
|
|
|
|
|
CATEGORY I |
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(packings, gaskets, resilient/vinyl/asphalt) |
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
DESCRIBE MATERIAL TO BE |
|
TSI |
|
|
Ceiling |
|
VAT |
Transite |
Piping |
|
Type of |
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
||||||||||||||||||||||
|
REMOVED |
|
|
|
Fireproofing |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
VAT |
|
Asphalt Roofing |
|
|
||||
|
|
|
|
|
Other______________ |
|
Other_____________ |
|
|
|
|
Other_________________ |
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
RACM - UNIT OF MEASUREMENT |
|
Linear Ft. |
|
Square Ft. |
|
Total Volume of all RACM |
|
Amount of |
|
|
||||||||||||||||||
|
(Type in Amount) |
|
|
|
|
|
|
|
|
|
|
|
|
|
_____________ Cubic Yards (mandatory) |
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
VI. FACILITY INFORMATION *
Owner Name:
Contact Name:
Telephone No.
Fax No.
Mailing Address:
City:
State:
Zip Code:
Email:
VII. ASBESTOS REMOVAL CONTRACTOR INFORMATION FOR RACM
Asbestos Removal Contractor Name: |
|
LA Contractor’s License |
||||||
|
|
|
No. |
|
|
|
|
|
Mailing Address: |
|
Fax No. |
Contact: |
Supervisor Exp. Date: |
||||
|
|
|
( |
) |
|
|
|
|
City: |
|
State: |
|
|
Zip Code: |
Telephone No. |
Email: |
|
|
|
|
|
|
|
( |
) |
|
VIII. OTHER OPERATOR/DEMOLITION CONTRACTOR: *
Contact:
Telephone No. ( |
) |
Mailing Address:
City:
State:
Zip Code:
Email:
IX. SCHEDULED DATES ASBESTOS REMOVAL (MM/DD/YY)
Start:
Complete:
X. SCHEDULED DEMO/RENOVATION DATES (MM/DD/YY)*
Start:
Complete:
Form_7077_r03 9/15/11
NOTIFICATION OF DEMOLITION AND RENOVATION FORM –
XI. SOLID WASTE TRANSPORTER TO LANDFILL FOR RACM
|
Name: |
|
DEQ SW Transporter No. |
Contact: |
|
Telephone No. |
|||
|
|
|
|
|
|
( |
) |
|
|
|
Address: |
|
City: |
State: |
Zip Code: |
Email: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
XII. SOLID WASTE TRANSPORTER ONLY IF TAKEN TO OFFSITE PREMISES AND STORED PRIOR TO DISPOSAL (RACM ONLY) |
||||||||
|
Name: |
DEQ SW Transporter No. |
Contact: |
|
Telephone No. |
||||
|
|
|
|
|
|
( |
) |
|
|
|
Address: |
|
|
City: |
|
State: |
|
Zip Code: |
|
|
|
|
|
|
|
|
|
|
|
Physical Location of Drop Off Area:
City:
State:
XIII. ASBESTOS WASTE DISPOSAL SITE FOR RACM:
|
Name: |
Contact: |
Telephone No. |
|||
|
|
|
( |
) |
|
|
|
Physical Location: |
City: |
State: |
|
Zip Code: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
XIV. IF DEMOLITION ORDERED BY A GOVERNMENT AGENCY, PLEASE IDENTIFY THE AGENCY REPRESENATIVE:
|
Name: |
Title: |
Authority: |
|
|
|
|
|
|
|
Date of Order: (MM/DD/YY) |
Date Ordered To Begin: (MM/DD/YY) |
Note: Copy of Order must be attached to this |
|
|
|
|
Notification. |
|
|
|
|
|
|
XV. EMERGENCY RENOVATIONS INVOLVING RACM:
Date |
and |
Hour |
of |
Emergency: |
Description of the Sudden, Unexpected Event that must immediately be attended to: |
(MM/DD/YY) |
|
|
|
|
|
|
|
|
|
|
|
Section 5151.F.2.d.xv – Explain how the event caused an unsafe condition (or health hazard) or would cause equipment damage, or poses an unreasonable financial burden:
Section 5151.F.2.d.xv
XVI. Description of planned
XVII. I certify that the above information is correct and that personnel performing asbestos Demolition or Renovation activities are trained and accredited in accordance with LAC 33:III.5151; and that the evidence of the required training will be available on the project site for inspection by LDEQ personnel. (Sign Sec. XVII only if RACM is present)
____________________ |
__________________________________________ |
______________________ |
(Date) |
(Signature of Owner or Operator/Contractor) |
(Printed Name) |
XVIII. * Certify in this Section For Demolitions Only if the Structure Contains No Regulated Asbestos Containing Material (RACM) I certify that the above information is correct and that during Demolition No Regulated Asbestos Containing Material is present.
____________________ |
__________________________________________ |
______________________ |
|
|
||
|
(Date) |
|
(Signature of Owner or Operator/Contractor) |
(Printed Name) |
|
|
|
|
|
|
|
|
|
|
ADVF Fees: |
$66 |
(Minimum of 10 working days notification given) |
|
|
|
|
|
$99 |
for Emergencies (less than 10 working days notification given) No Voucher’s Will Be Accepted for Emergencies |
|
||
|
|
*No Fee for Notification of Demo containing No RACM (Negative Declaration) may be faxed – Fax # |
|
|||
REMIT TO: LDEQ / OES – Permit Support Services Division, Notif & Accred Section, P. O. BOX 4313, BATON ROUGE, LA
Pursuant to La. R.S. 40.1574 A&B, be advised that no construction or renovation can begin until the plans and specifications are reviewed by the Office of the State Fire Marshall or it is determined by that Office that plans are not required to be submitted.
Form_7077_r03 6/09/10
Page 2 of 2