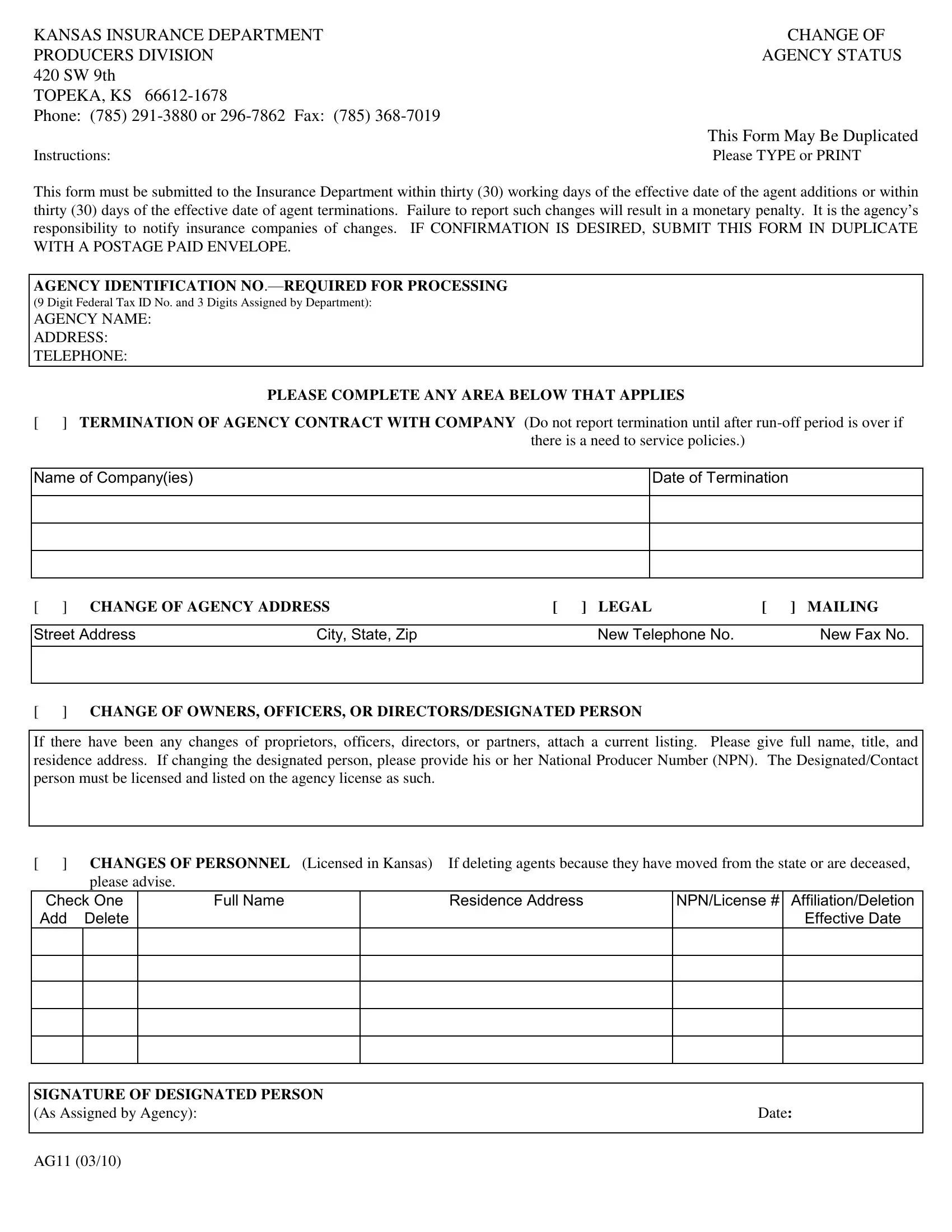
The Ag11 form, a critical document issued by the Kansas Insurance Department, plays a pivotal role in maintaining the accuracy of agency records within the state's insurance industry. Each change in an agency’s status, whether it involves adding new agents, the termination of agents, changes in agency address, or updates in ownership, officers, or designated personnel, must be reported using this form. Agencies are given a narrow window of thirty working days from the effective date of these changes to submit the form, failing which they could face monetary penalties. This underscores the form’s significance in ensuring that the department's records are current, which in turn facilitates the smooth operation of insurance services in Kansas. Furthermore, the Ag11 form serves as a communication tool between the agency and insurance companies, notifying them of pertinent changes that could affect their operations. The detailed instructions provided with the form stress the importance of accuracy and timeliness, with the option to receive confirmation by submitting the document in duplicate along with a postage-paid envelope. Agencies are required to provide comprehensive information including their identification number, any personnel changes, and updated contact details, ensuring that the insurance department and associated companies remain well-informed about the agency’s current status.
| Question | Answer |
|---|---|
| Form Name | Form Ag11 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | kansas insurance dep ag11, kansas insurance dpeartment form ag11, ag11 form kansas, kansas ag11 form |
KANSAS INSURANCE DEPARTMENT |
CHANGE OF |
PRODUCERS DIVISION |
AGENCY STATUS |
420 SW 9th |
|
TOPEKA, KS |
|
Phone: (785) |
|
|
This Form May Be Duplicated |
Instructions: |
Please TYPE or PRINT |
This form must be submitted to the Insurance Department within thirty (30) working days of the effective date of the agent additions or within thirty (30) days of the effective date of agent terminations. Failure to report such changes will result in a monetary penalty. It is the agency’s
responsibility to notify insurance companies of changes. IF CONFIRMATION IS DESIRED, SUBMIT THIS FORM IN DUPLICATE WITH A POSTAGE PAID ENVELOPE.
AGENCY IDENTIFICATION
(9 Digit Federal Tax ID No. and 3 Digits Assigned by Department):
AGENCY NAME:
ADDRESS:
TELEPHONE:
PLEASE COMPLETE ANY AREA BELOW THAT APPLIES
[ ] TERMINATION OF AGENCY CONTRACT WITH COMPANY (Do not report termination until after
Name of Company(ies)
Date of Termination
[ ] CHANGE OF AGENCY ADDRESS |
[ ] LEGAL |
[ ] MAILING |
|
|
|
|
|
Street Address |
City, State, Zip |
New Telephone No. |
New Fax No. |
|
|
|
|
|
|
|
|
[ ] CHANGE OF OWNERS, OFFICERS, OR DIRECTORS/DESIGNATED PERSON
If there have been any changes of proprietors, officers, directors, or partners, attach a current listing. Please give full name, title, and residence address. If changing the designated person, please provide his or her National Producer Number (NPN). The Designated/Contact person must be licensed and listed on the agency license as such.
[ ] CHANGES OF PERSONNEL (Licensed in Kansas) If deleting agents because they have moved from the state or are deceased, please advise.
Check One
Add Delete
Full Name
Residence Address
NPN/License # Affiliation/Deletion Effective Date
SIGNATURE OF DESIGNATED PERSON |
|
(As Assigned by Agency): |
Date: |
AG11 (03/10)