
By using the online editor for PDFs by FormsPal, it is easy to complete or modify usaid form right here. The editor is continually updated by our team, getting powerful functions and growing to be a lot more convenient. To get the process started, consider these easy steps:
Step 1: Press the "Get Form" button above. It'll open up our editor so that you could start completing your form.
Step 2: This tool offers the capability to customize almost all PDF documents in various ways. Enhance it by adding any text, correct what is originally in the PDF, and put in a signature - all possible within a few minutes!
It is actually an easy task to fill out the pdf following our helpful tutorial! Here's what you need to do:
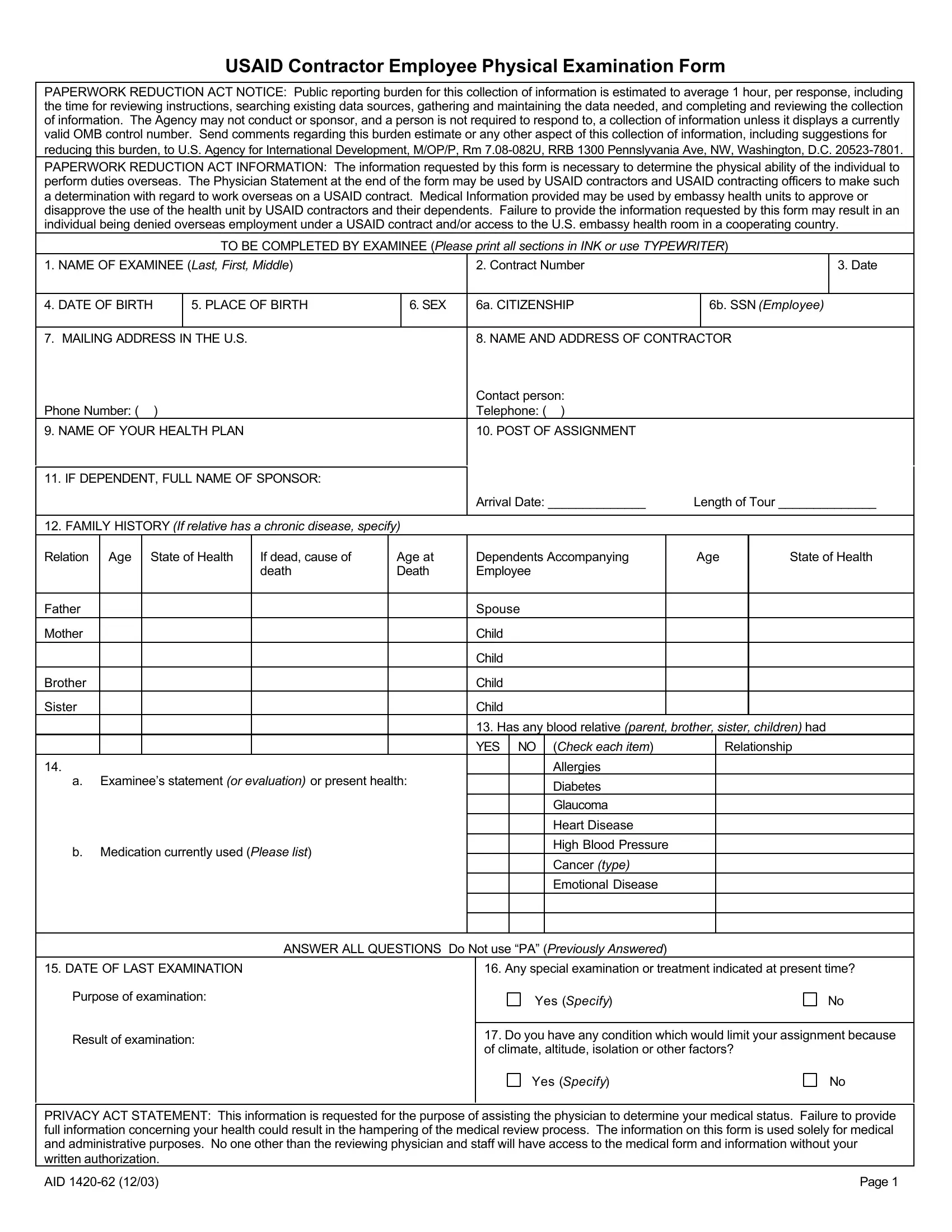
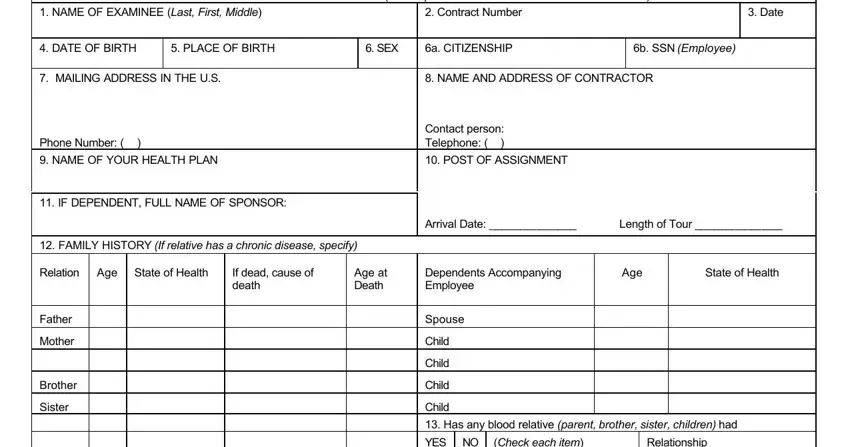
1. The usaid form involves specific details to be inserted. Make sure the following fields are completed:
2. After filling out the last section, head on to the subsequent stage and fill out all required details in all these blanks - a Examinees statement or, b Medication currently used Please, YES NO, Check each item, Relationship, Allergies, Diabetes, Glaucoma, Heart Disease, High Blood Pressure, Cancer type, Emotional Disease, DATE OF LAST EXAMINATION, Any special examination or, and ANSWER ALL QUESTIONS Do Not use PA.
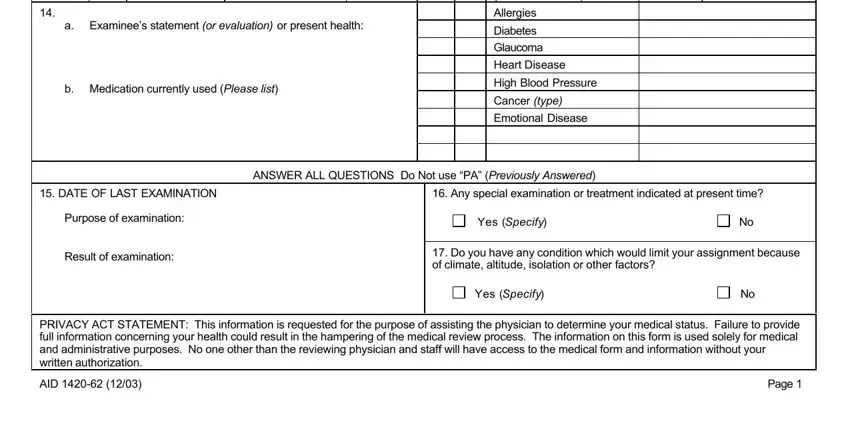
Concerning YES NO and Emotional Disease, make sure you take a second look here. These are definitely the most significant ones in this document.
3. The following section will be focused on Have you had any significant, Have you ever been a patient in a, Have you been denied life, DO YOU NOW HAVE OR HAVE YOU EVER, YES, Check each item, YES, Check each item, Frequent or severe headaches, Kidney trouble stone or blood, Recent gain or loss of weight, and Tuberculosis or close association - fill in every one of these empty form fields.
4. This specific section comes next with the following blanks to fill out: Tuberculosis or close association, High blood pressure, Frequent trouble sleeping Nervous, Frequent indigestion Stomach liver, Specify any GYN surgery or disease, Date of last Menses, FEMALES ONLY, Excessive bleeding after injury or, Do you use any medication, I CERTIFY THAT I HAVE READ THE, SIGNATURE OF EXAMINEE, DATE, and NOTE For the Examining Physician.
5. The last point to conclude this document is pivotal. You'll want to fill in the appropriate blank fields, and this includes SIGNIFICANT ANDOR INTERVAL, AID, and Page, prior to using the document. Failing to do this could produce an unfinished and potentially unacceptable paper!
Step 3: As soon as you have glanced through the information in the document, simply click "Done" to conclude your form at FormsPal. Sign up with FormsPal today and immediately access usaid form, available for download. Every single modification made is handily preserved , which means you can edit the pdf later if required. At FormsPal.com, we aim to guarantee that all your information is stored protected.