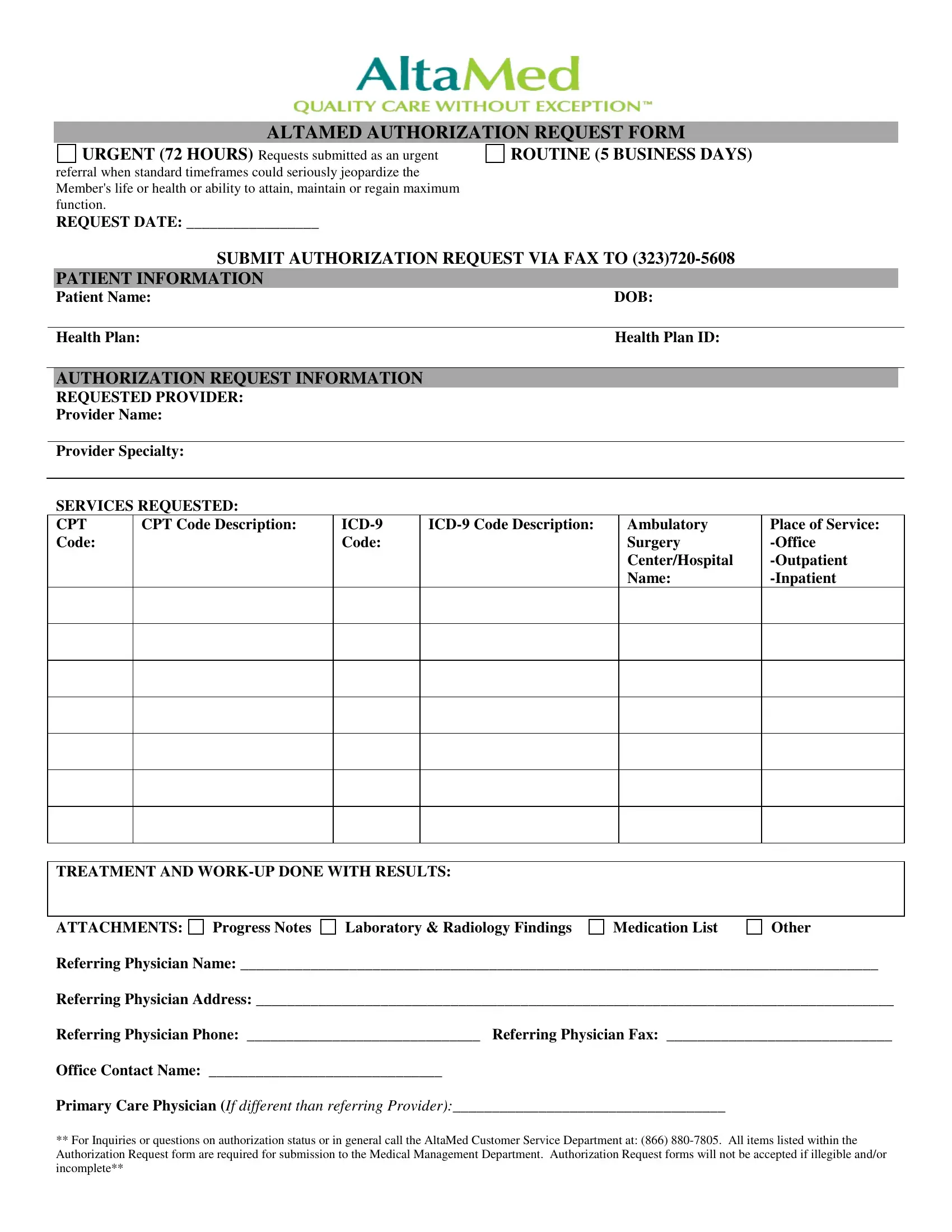
Navigating through healthcare procedures requires understanding various forms, among which the AltaMed Authorization Request Form stands pivotal for patients requiring timely medical attention. This essential document bridges the gap between patients and the necessary healthcare services, categorizing requests into 'urgent' and 'routine' to streamline prioritization based on the severity of the patient's condition. Urgent requests are marked for situations where a delay could critically affect the patient's well-being, demanding a swift response within 72 hours. Conversely, routine requests are processed within five business days. The form meticulously gathers patient information, including name, date of birth, health plan, and health plan ID. It ensures that healthcare providers have a complete overview by requesting details on the requested services, including provider name and specialty, service descriptions via CPT and ICD-9 codes, and preferred service locations. It also emphasizes a thorough documentation of the patient's medical history, such as treatment and work-up results, along with any relevant attachments like progress notes or medication lists. To ensure the request's smooth processing, the form mandates contact details of the referring physician and an office contact. For additional support, the AltaMed Customer Service Department is ready to assist with inquiries, underlining the importance of a fully completed and legible form to expedite the authorization process.
| Question | Answer |
|---|---|
| Form Name | AltaMed Authorization Form |
| Form Length | 1 pages |
| Fillable? | Yes |
| Fillable fields | 61 |
| Avg. time to fill out | 12 min 31 sec |
| Other names | altamed auth form, altamed doctors note, altamed authorization form, altamed form get |
ALTAMED AUTHORIZATION REQUEST FORM
URGENT (72 HOURS) Requests submitted as an urgent referral when standard timeframes could seriously jeopardize the Member's life or health or ability to attain, maintain or regain maximum function.
ROUTINE (5 BUSINESS DAYS)
REQUEST DATE: _________________
SUBMIT AUTHORIZATION REQUEST VIA FAX TO
PATIENT INFORMATION
Patient Name: |
DOB: |
|
|
Health Plan: |
Health Plan ID: |
AUTHORIZATION REQUEST INFORMATION
REQUESTED PROVIDER:
Provider Name:
Provider Specialty:
SERVICES REQUESTED:
CPT Code:
CPT Code Description:
Ambulatory
Surgery
Center/Hospital
Name:
Place of Service:
TREATMENT AND
ATTACHMENTS: Progress Notes |
Laboratory & Radiology Findings |
Medication List |
Other |
Referring Physician Name: __________________________________________________________________________________
Referring Physician Address: __________________________________________________________________________________
Referring Physician Phone: ______________________________ Referring Physician Fax: _____________________________
Office Contact Name: ______________________________
Primary Care Physician (If different than referring Provider):___________________________________
**For Inquiries or questions on authorization status or in general call the AltaMed Customer Service Department at: (866)