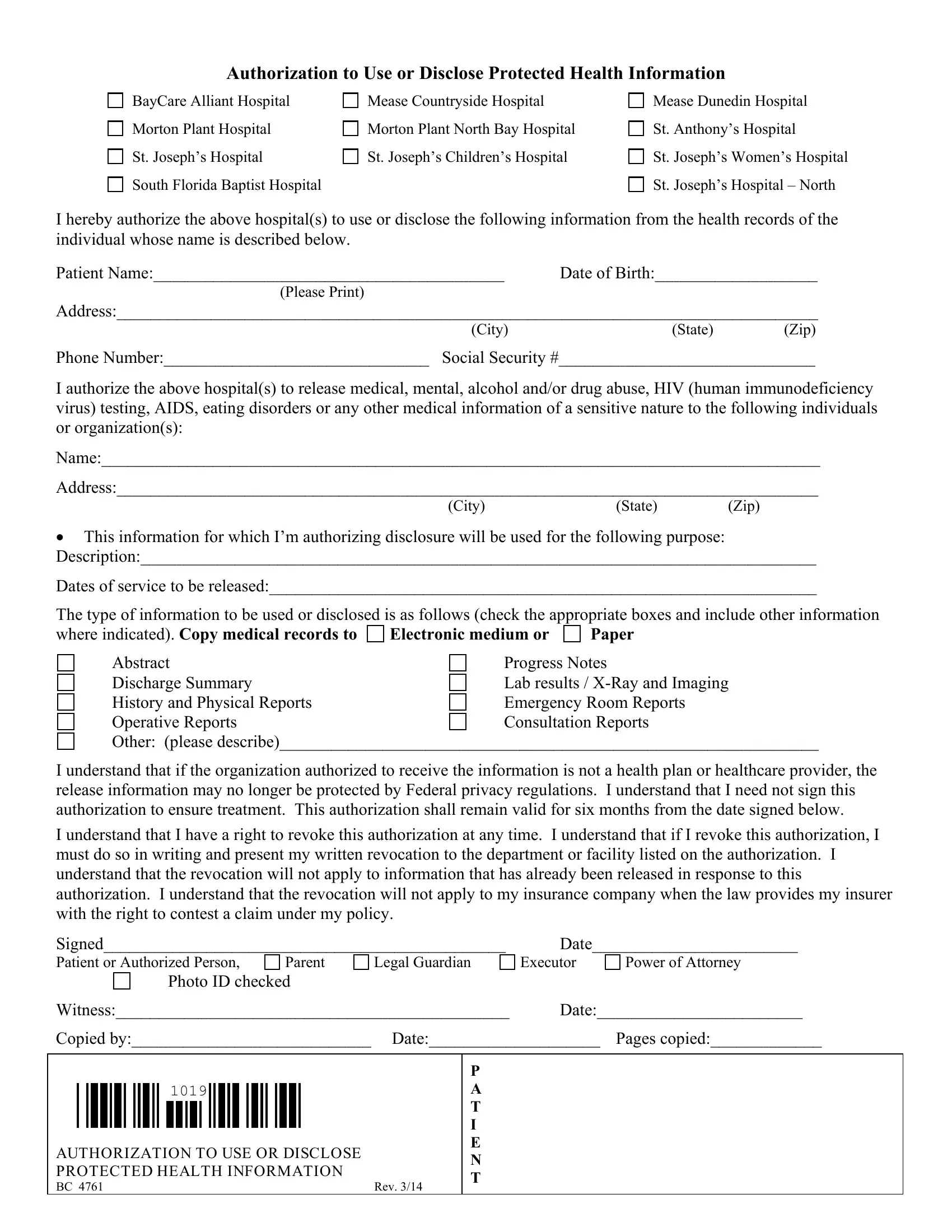
At the heart of maintaining patient privacy and ensuring the controlled sharing of health information are forms like BC 4761, a crucial document implemented by a network of hospitals including BayCare Alliant Hospital, Morton Plant Hospital, and several others across the region. This form, titled "Authorization to Use or Disclose Protected Health Information," serves as a written permission slip from a patient or an authorized person, allowing specific health details to be shared with named individuals or organizations for clearly stated purposes. It covers a wide range of medical data, including sensitive information related to mental health, HIV/AIDS status, substance abuse, and more. By selecting from a variety of record types—ranging from medical records in electronic or paper form to detailed operative and consultation reports—patients can control what aspects of their health history are disclosed. Moreover, the form highlights the voluntary nature of this authorization, reassuring patients that their treatment will not be affected by their decision to grant or withhold consent. It remains valid for six months, giving patients the flexibility to revoke authorization at any time with a written notice, though it clarifies that revocation won't affect already shared information or disclosures made to insurers under legal obligations. Such documents not only empower patients in managing their health information but also underscore the hospitals' commitment to respecting patient privacy in accordance with federal regulations.
| Question | Answer |
|---|---|
| Form Name | Form Bc 4761 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | Anthonys, bc 4761, HIV, Josephs |
Authorization to Use or Disclose Protected Health Information
BayCare Alliant Hospital
Morton Plant Hospital
St. Joseph’s Hospital
South Florida Baptist Hospital
Mease Countryside Hospital
Morton Plant North Bay Hospital
St. Joseph’s Children’s Hospital
Mease Dunedin Hospital
St. Anthony’s Hospital
St. Joseph’s Women’s Hospital
St. Joseph’s Hospital – North
I hereby authorize the above hospital(s) to use or disclose the following information from the health records of the individual whose name is described below.
Patient Name:_________________________________________ |
Date of Birth:___________________ |
|
(Please Print) |
|
|
Address:__________________________________________________________________________________ |
||
(City) |
(State) |
(Zip) |
Phone Number:_______________________________ Social Security #______________________________
I authorize the above hospital(s) to release medical, mental, alcohol and/or drug abuse, HIV (human immunodeficiency virus) testing, AIDS, eating disorders or any other medical information of a sensitive nature to the following individuals or organization(s):
Name:____________________________________________________________________________________
Address:__________________________________________________________________________________
(City) |
(State) |
(Zip) |
•This information for which I’m authorizing disclosure will be used for the following purpose: Description:_______________________________________________________________________________
Dates of service to be released:________________________________________________________________
The type of information to be used or disclosed is as follows (check the appropriate boxes and include other information
where indicated). Copy medical records to |
Electronic medium or |
Paper |
Abstract |
Progress Notes |
|
Discharge Summary |
Lab results / |
|
History and Physical Reports |
Emergency Room Reports |
|
Operative Reports |
Consultation Reports |
|
Other: (please describe)_______________________________________________________________
I understand that if the organization authorized to receive the information is not a health plan or healthcare provider, the release information may no longer be protected by Federal privacy regulations. I understand that I need not sign this authorization to ensure treatment. This authorization shall remain valid for six months from the date signed below.
I understand that I have a right to revoke this authorization at any time. I understand that if I revoke this authorization, I must do so in writing and present my written revocation to the department or facility listed on the authorization. I understand that the revocation will not apply to information that has already been released in response to this authorization. I understand that the revocation will not apply to my insurance company when the law provides my insurer with the right to contest a claim under my policy.
Signed_______________________________________________
Patient or Authorized Person, |
Parent |
Legal Guardian |
Photo ID checked Witness:______________________________________________
Date________________________
Executor |
Power of Attorney |
Date:________________________
Copied by:____________________________ Date:____________________ Pages copied:_____________
1019
AUTHORIZATION TO USE OR DISCLOSE PROTECTED HEALTH INFORMATION
BC 4761 |
Rev. 3/14 |
P A T I E N T