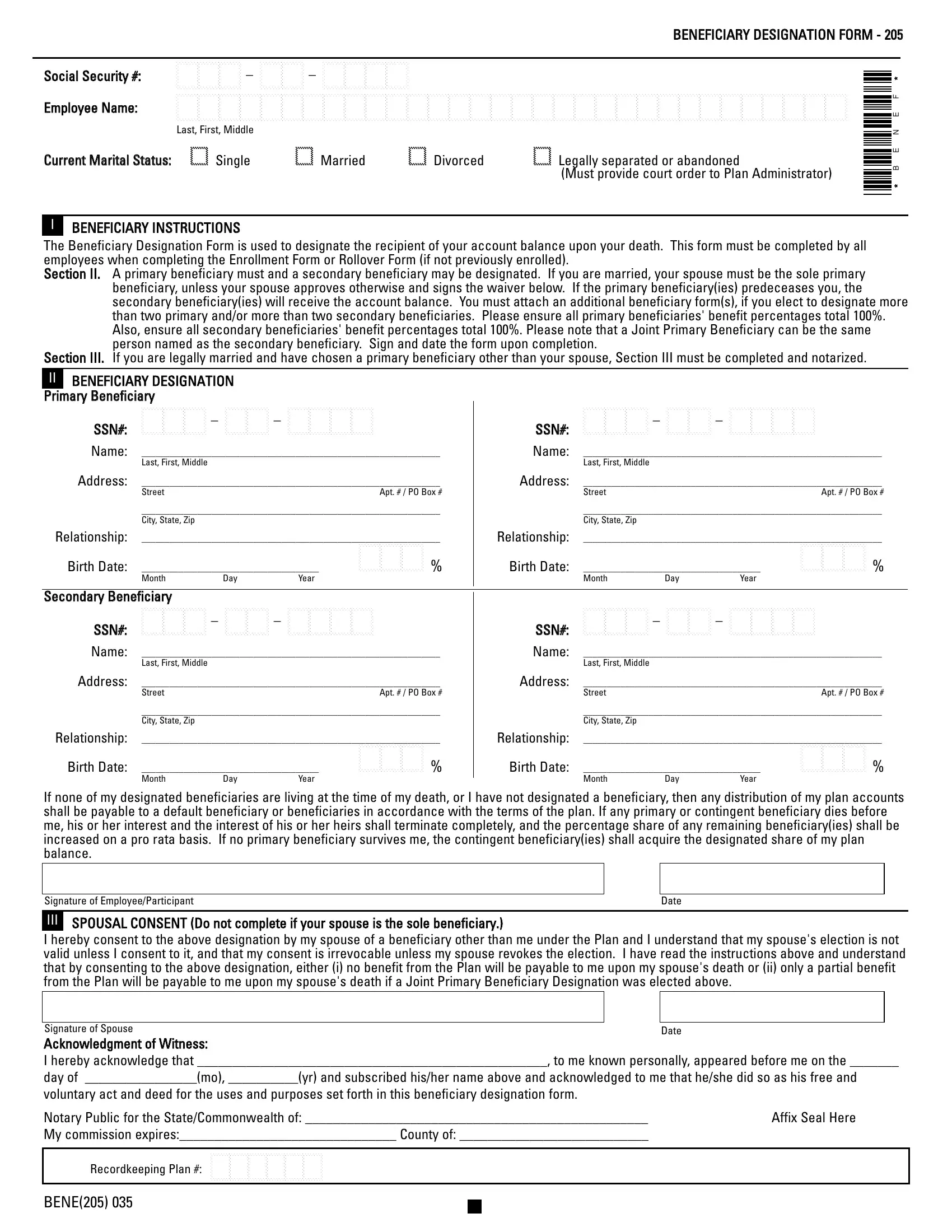
The Bene 205 form, a crucial document for employees, plays an instrumental role in delineating the fate of an account balance after the account holder's demise. This Beneficiary Designation Form requires meticulous completion alongside or subsequent to Enrollment or Rollover Forms, ensuring employees make clear decisions regarding their primary and secondary beneficiaries. The form uniquely stipulates that for married employees, the spouse is automatically the primary beneficiary unless a waiver is signed, illustrating the legal safeguards around marital finances. Additionally, it allows for the designation of both primary and secondary beneficiaries, mandating that their benefit percentages collectively reach 100%. This requirement ensures a clear division of assets, preventing potential disputes among beneficiaries. Provision is also made for situations where a chosen beneficiary predeceases the employee or if no beneficiary is designated at all, detailing how the account balance should be distributed in such instances. The form incorporates a section specifically for married employees who wish to nominate someone other than their spouse as a primary beneficiary, necessitating notarized spousal consent to underline the importance of this choice. The intricate balance between respecting an employee's beneficiary choices and protecting spousal rights underlines the form’s significance in financial and estate planning.
| Question | Answer |
|---|---|
| Form Name | Form Bene 205 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | NJ, formNOT, predeceases, adp nj crs newark nj |
BENEFICIARY DESIGNATION FORM - 205
Social Security #: |
|
Employee Name: |
!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!! |
|
Last, First, Middle |
Current Marital Status: |
! Single! Married! Divorced! Legally separated or abandoned |
|
(Must provide court order to Plan Administrator) |
IBENEFICIARY INSTRUCTIONS
*BENEF*
The Beneficiary Designation Form is used to designate the recipient of your account balance upon your death. This form must be completed by all employees when completing the Enrollment Form or Rollover Form (if not previously enrolled).
Section II. A primary beneficiary must and a secondary beneficiary may be designated. If you are married, your spouse must be the sole primary beneficiary, unless your spouse approves otherwise and signs the waiver below. If the primary beneficiary(ies) predeceases you, the secondary beneficiary(ies) will receive the account balance. You must attach an additional beneficiary form(s), if you elect to designate more than two primary and/or more than two secondary beneficiaries. Please ensure all primary beneficiaries' benefit percentages total 100%. Also, ensure all secondary beneficiaries' benefit percentages total 100%. Please note that a Joint Primary Beneficiary can be the same person named as the secondary beneficiary. Sign and date the form upon completion.
Section III. If you are legally married and have chosen a primary beneficiary other than your spouse, Section III must be completed and notarized.
IIBENEFICIARY DESIGNATION Primary Beneficiary
SSN#: |
SSN#: |
||||||||
Name: |
________________________________________________________________ |
Name: |
________________________________________________________________ |
||||||
|
Last, First, Middle |
|
|
|
|
Last, First, Middle |
|
|
|
Address: |
________________________________________________________________ |
Address: |
________________________________________________________________ |
||||||
|
Street |
|
|
Apt. # / PO Box # |
|
Street |
|
|
Apt. # / PO Box # |
|
________________________________________________________________ |
|
________________________________________________________________ |
||||||
|
City, State, Zip |
|
|
|
|
City, State, Zip |
|
|
|
Relationship: |
________________________________________________________________ |
Relationship: |
________________________________________________________________ |
||||||
Birth Date: |
______________________________________ |
!!! % |
Birth Date: |
______________________________________ |
!!! % |
||||
|
Month |
Day |
Year |
|
|
Month |
Day |
Year |
|
Secondary Beneficiary |
|
|
|
|
SSN#: |
||||
Name: |
________________________________________________________________ |
|||
|
Last, First, Middle |
|
|
|
Address: |
________________________________________________________________ |
|||
|
Street |
|
|
Apt. # / PO Box # |
|
________________________________________________________________ |
|||
|
City, State, Zip |
|
|
|
Relationship: |
________________________________________________________________ |
|||
Birth Date: |
______________________________________ |
!!! % |
||
|
Month |
Day |
Year |
|
SSN#:
Name: |
________________________________________________________________ |
|||
|
Last, First, Middle |
|
|
|
Address: |
________________________________________________________________ |
|||
|
Street |
|
|
Apt. # / PO Box # |
|
________________________________________________________________ |
|||
|
City, State, Zip |
|
|
|
Relationship: |
________________________________________________________________ |
|||
Birth Date: |
______________________________________ |
!!! % |
||
|
Month |
Day |
Year |
|
If none of my designated beneficiaries are living at the time of my death, or I have not designated a beneficiary, then any distribution of my plan accounts shall be payable to a default beneficiary or beneficiaries in accordance with the terms of the plan. If any primary or contingent beneficiary dies before me, his or her interest and the interest of his or her heirs shall terminate completely, and the percentage share of any remaining beneficiary(ies) shall be increased on a pro rata basis. If no primary beneficiary survives me, the contingent beneficiary(ies) shall acquire the designated share of my plan balance.
Signature of Employee/Participant |
Date |
III
SPOUSAL CONSENT (Do not complete if your spouse is the sole beneficiary.)
I hereby consent to the above designation by my spouse of a beneficiary other than me under the Plan and I understand that my spouse's election is not valid unless I consent to it, and that my consent is irrevocable unless my spouse revokes the election. I have read the instructions above and understand that by consenting to the above designation, either (i) no benefit from the Plan will be payable to me upon my spouse's death or (ii) only a partial benefit from the Plan will be payable to me upon my spouse's death if a Joint Primary Beneficiary Designation was elected above.
|
|
|
Signature of Spouse |
|
Date |
Acknowledgment of Witness: |
|
|
I hereby acknowledge that __________________________________________________, to me known personally, appeared before me on the _______
day of ________________(mo), __________(yr) and subscribed his/her name above and acknowledged to me that he/she did so as his free and
voluntary act and deed for the uses and purposes set forth in this beneficiary designation form.
Notary Public for the State/Commonwealth of: _________________________________________________ |
Affix Seal Here |
My commission expires:_______________________________ County of: ___________________________ |
|
Recordkeeping Plan #: !!!!!!1 2 3 4 5 6
BENE(205) 035