Instructions for Application for Fire Safety Plan Examination
To Expedite Your Review:
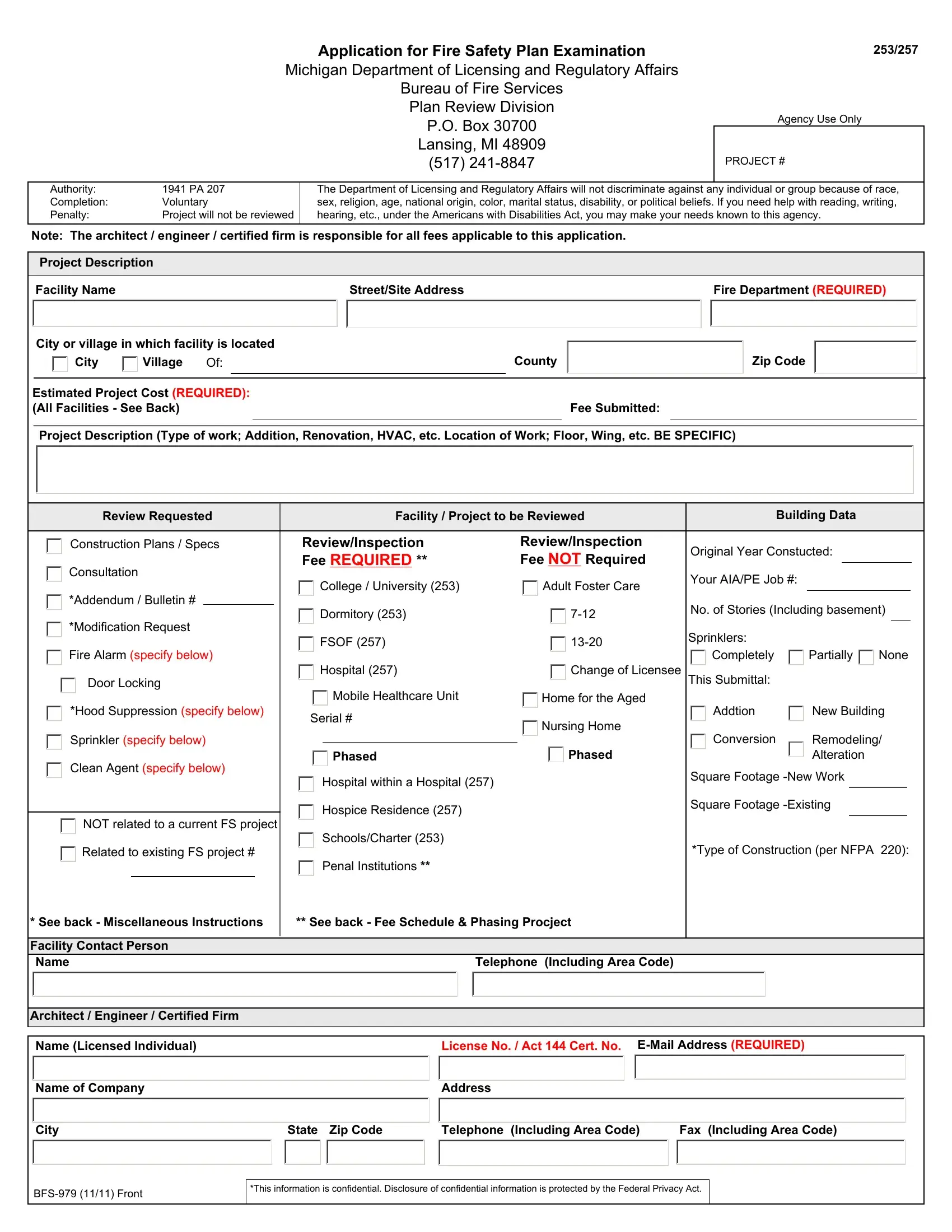
-All submittals must be accompanied by an Application for Fire Safety Plan Review completely filled out. -Provide all requested information.
-An "n/a" designation is helpful for areas where information does not pertain to the project.
-Only ONE set of construction documents or related specification drawings is required.
-Construction documents must be signed and sealed by an architect or professional engineer licensed in the State of Michigan as required by 1980 PA 299.
-Fire Suppression and fire alarm shop drawings and computations are not required to be sealed by a design professional.
-Act 144 certified firms shall provide the certification number issued by the Bureau of Fire Services.
-All fees are due upon submittal (colleges, hospitals, universities, dormitories, schools, charter, schools, hospice residences, FSOF, and penal institutions submitted by a non-state agency).
**Fees are applicable on construction documents, fire alarm, door locking, sprinkler, hood suppression, and clean agent suppression system shop drawings in colleges, dormitories, free-standing outpatient facilities/ambulatory surgical centers, hospitals, universities, schools, charter schools, hospice residences, and penal institutions (submitted by a non-state agency).
Fees are not assessed for any other type of facilities, including penal institutions when submitted by a state agency.
-All floor plans shall indicate exit locations, identify all room uses, and sprinkler coverage, if any.
-Furnish approved design numbers of all fire related assemblies.
-Changes to previously reviewed drawings must be specifically brought to our attention for review and comment.
-Submit a seperate check or money order for each project payable to the State of Michigan.
-Health Care Project: When applicable, identify the area(s) occupied by ambulatory/non-ambulatory patients, outpatients, and location of all smoke barriers.
-Architect / Engineer / Certified Firm: Provide all requested information. All correspondence will be sent to this e-mail address and this entity will be responsible for all fees.
Note: A hold will be placed on any project with fees owed. The project will not be sent to our field office and inspections will not take place until all fees have been paid.
**Fee Schedule
(Free-standing outpatient facilities and hospitals; colleges, universities, dormitories, schools, charter schools, hospice residences, and
penal institutions**)
Project Cost Range |
Fee |
$101,000.00 or less |
Minimum fee of $155.00 |
$101,001.00 to 1,500,000.00 |
$1.60 per $1,000.00 |
$1,500,001.00 to 10,000,000.00 |
$1.30 per $1,000.00 |
$10,000,001.00 or more |
$1.10 per $1,000.00 - Maximum fee $60,000 |
Estimated Project Cost (if original plans/specs): The Project Cost includes all costs associated with the project other than the cost of equipment that is not
"fixed'. "Fixed" equipment is defined as equipment necessary to the operation of the building, including but not limited to: air handlers, boilers, chillers, electrical switchgear, elevators, generators, modular casework, etc. If labor is being provided for the project, the cost of the labor shall be included.
*Miscellaneous Instructions
Phased Projects- A phased project is a project that requires areas to be occupied before the over all project is completed. Phased projects require a seperate application and submittal for each phase. Costs & fees shall be applied per phase. We will treat each phase with a seperate project # so the coordination with Act 144 Certified Firms will be the responsibility of the Architect.
-Hood suppression systems shall be reviewed and billed individually.
-Review of modifications, addenda, and bulletins shall be billed $155.00 for application with a one-hour review. All review time after first hour is to be billed at $50.00 per hour.
-Plan review consultation has a flat fee of $155.00.
-Modification Requests are defined as a request to a modification of a rule or section of the code.
Project Description: Please indicate floor or work site to assist in identifying the project location, as well as:
Square footage of new building, addition, remodeling, etc; Square footage of an existing building; Project Scope (description of project)
Type of Review Requested: If the review you are requesting in not on the form, please write in your request.
Type of Construction (per NFPA 220): Below is a cross-reference chart of Building Construction Types
NFPA 220 |
I(442) |
I(332) |
II(222) |
II(111) |
II(000) |
III(211) |
III(200) |
IV(2HH) |
V(111) |
V(000) |
MBC |
- |
IA |
IB |
IIA |
IIB |
IIIA |
IIIB |
IVHT |
VA |
VB |