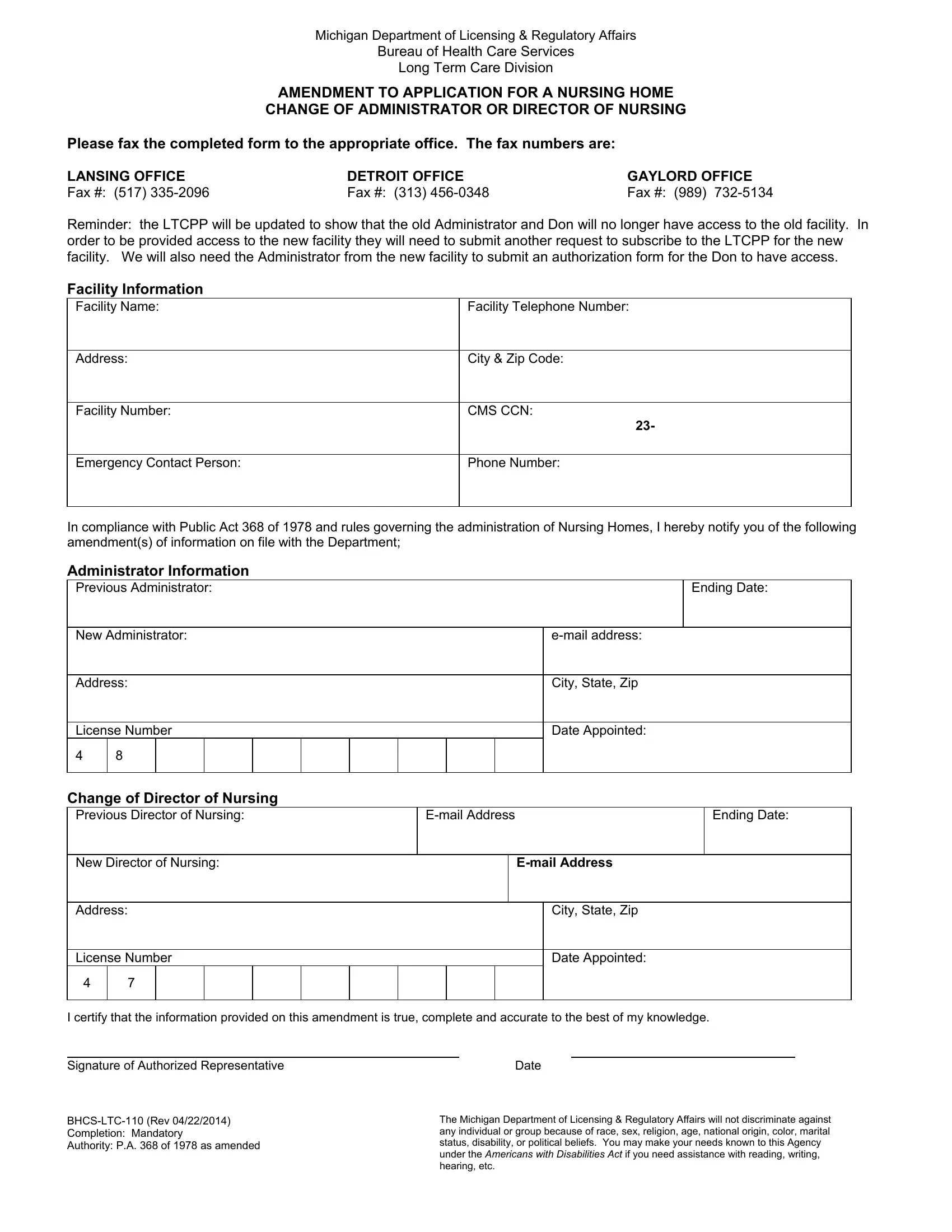
In the realm of long-term care facilities, ensuring smooth transitions during changes in leadership positions such as administrators or directors of nursing is crucial for maintaining the quality of care and operational continuity. The Michigan Department of Licensing & Regulatory Affairs, through its Bureau of Health Care Services Long Term Care Division, facilitates these transitions via the BHCS LTC 110 form. This pivotal document serves as an amendment to the application for a nursing home change, specifically when there's a change of administrator or director of nursing. The form requires comprehensive information about the facility, including its name, address, facility number, and emergency contact details, alongside the critical CMS CCN. It also captures detailed information about the outgoing and incoming administrators or directors of nursing, ranging from their names and email addresses to license numbers and appointment dates. As a mandate, the form requires the signature of an authorized representative, attesting to the accuracy and completeness of the information provided. It highlights the seamless process for updating access permissions within the Long-Term Care Provider Portal (LTCPP) for administrators and directors of nursing, ensuring that only authorized individuals have access to sensitive facility and patient information. Additionally, the document underscores the Michigan Department of Licensing & Regulatory Affairs' commitment to non-discrimination and accessibility, adhering to the Americans with Disabilities Act and offering support for individuals who require assistance.
| Question | Answer |
|---|---|
| Form Name | Form Bhcs Ltc 110 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | 1978, Saginaw, BHS, bhcs ltc 110 |
Michigan Department of Licensing & Regulatory Affairs
Bureau of Health Care Services
Long Term Care Division
AMENDMENT TO APPLICATION FOR A NURSING HOME
CHANGE OF ADMINISTRATOR OR DIRECTOR OF NURSING
Please fax the completed form to the appropriate office. The fax numbers are:
LANSING OFFICE |
DETROIT OFFICE |
GAYLORD OFFICE |
Fax #: (517) |
Fax #: (313) |
Fax #: (989) |
Reminder: the LTCPP will be updated to show that the old Administrator and Don will no longer have access to the old facility. In order to be provided access to the new facility they will need to submit another request to subscribe to the LTCPP for the new facility. We will also need the Administrator from the new facility to submit an authorization form for the Don to have access.
Facility Information
Facility Name:
Address:
Facility Number:
Facility Telephone Number:
City & Zip Code:
CMS CCN:
23-
Emergency Contact Person:
Phone Number:
In compliance with Public Act 368 of 1978 and rules governing the administration of Nursing Homes, I hereby notify you of the following amendment(s) of information on file with the Department;
Administrator Information
Previous Administrator: |
|
|
|
|
|
|
|
|
|
Ending Date: |
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
New Administrator: |
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Address: |
|
|
|
|
|
|
|
|
City, State, Zip |
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
License Number |
|
|
|
|
|
|
|
|
Date Appointed: |
||||||
4 |
8 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Change of Director of Nursing |
|
|
|
|
|
|
|
|
|
|
|
||||
Previous Director of Nursing: |
|
|
|
|
|
|
Ending Date: |
||||||||
|
|
|
|
|
|
|
|
|
|
||||||
New Director of Nursing: |
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
||||||
Address: |
|
|
|
|
|
|
|
|
City, State, Zip |
||||||
|
|
|
|
|
|
|
|
|
|
||||||
License Number |
|
|
|
|
|
|
|
|
Date Appointed: |
||||||
4 |
7 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
I certify that the information provided on this amendment is true, complete and accurate to the best of my knowledge.
Signature of Authorized Representative
Authority: P.A. 368 of 1978 as amended
Date
The Michigan Department of Licensing & Regulatory Affairs will not discriminate against any individual or group because of race, sex, religion, age, national origin, color, marital status, disability, or political beliefs. You may make your needs known to this Agency under the AMERICANS WITH DISABILITIES ACT if you need assistance with reading, writing, hearing, etc.