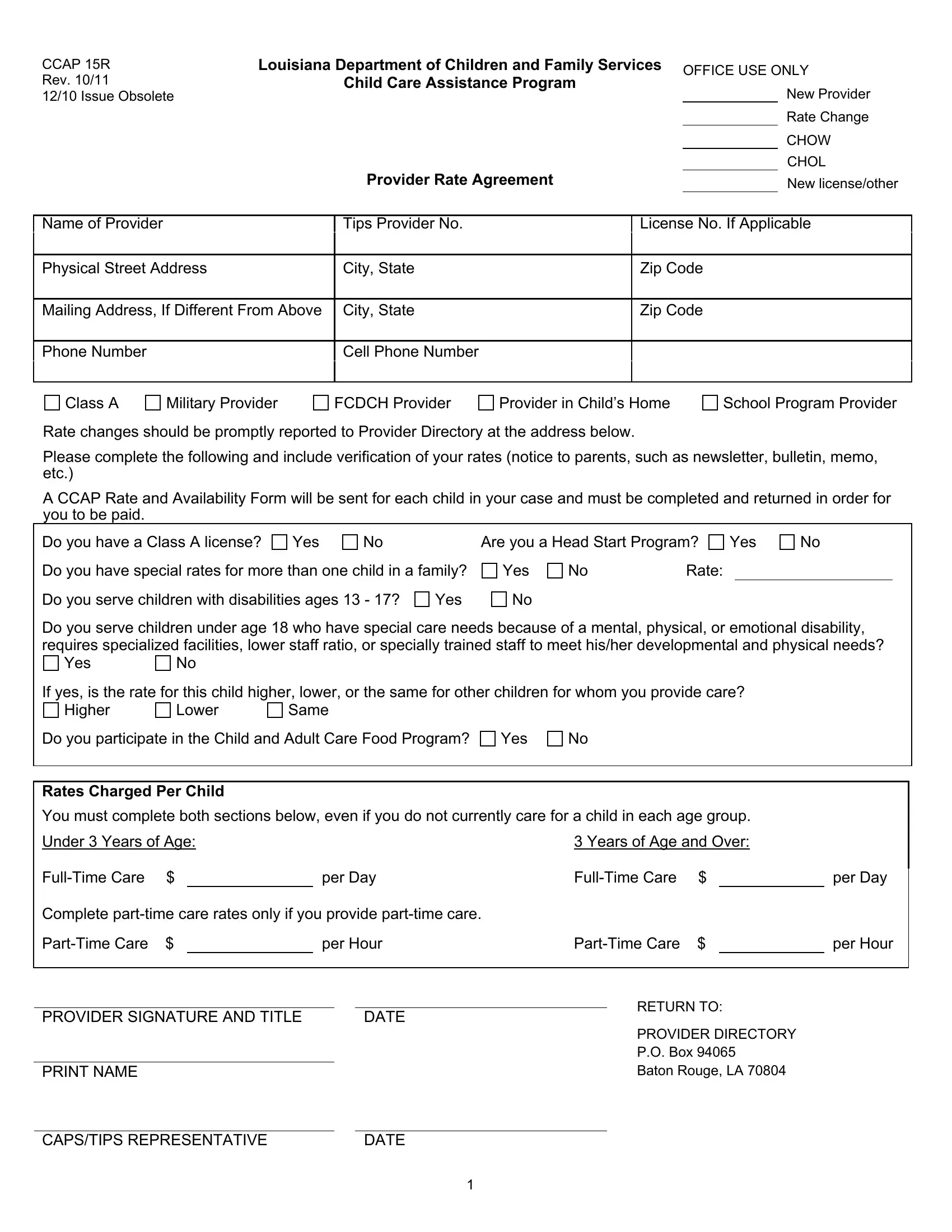
The CCAP 15R form is a crucial document for child care providers who are associated with or aim to become part of the Louisiana Department of Children and Family Services's Child Care Assistance Program (CCAP). This form plays a significant role whether a provider is stepping into the program anew, undergoing a rate change, navigating a Change of Ownership (CHOW), or undergoing changes in license or operational specifics. Mandating comprehensive information like the provider's name, contact details, licensing information, and service rates, the form facilitates transparent communication between providers and the CCAP. Providers are required to report any changes in their service rates promptly, ensuring that the assistance program remains updated. Furthermore, the form asks detailed questions regarding the provider's capabilities, such as whether they accommodate families with multiple children, children with disabilities, or those with special care needs, including the provision of services under the Child and Adult Care Food Program. Highlighting the importance of verifying one's rates through parent notices and the necessity of completing a CCAP Rate and Availability Form for each child under care, the CCAP 15R underscores its role as a vital instrument in maintaining the integrity and efficiency of child care services within Louisiana, ensuring that the program's financial assistance is accurately aligned with the providers' offerings.
| Question | Answer |
|---|---|
| Form Name | Form Ccap 15R |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | louisiana department of education ccap rate and availability verification form, louisiana child care assistance rates, ccap 10 form, child care assistance application form |
CCAP 15R |
Louisiana Department of Children and Family Services |
OFFICE USE ONLY |
|
Rev. 10/11 |
Child Care Assistance Program |
|
New Provider |
12/10 Issue Obsolete |
|
|
|
|
|
|
Rate Change |
|
|
|
CHOW |
|
|
|
CHOL |
|
Provider Rate Agreement |
|
New license/other |
Name of Provider
Tips Provider No.
License No. If Applicable
Physical Street Address
City, State
Zip Code
Mailing Address, If Different From Above
City, State
Zip Code
Phone Number
Cell Phone Number
Class A |
Military Provider |
FCDCH Provider |
Provider in Child’s Home |
School Program Provider |
Rate changes should be promptly reported to Provider Directory at the address below.
Please complete the following and include verification of your rates (notice to parents, such as newsletter, bulletin, memo, etc.)
A CCAP Rate and Availability Form will be sent for each child in your case and must be completed and returned in order for you to be paid.
Do you have a Class A license? |
Yes |
No |
|
Are you a Head Start Program? |
Yes |
No |
|||
Do you have special rates for more than one child in a family? |
Yes |
No |
Rate: |
|
|
|
|||
Do you serve children with disabilities ages 13 - 17? |
Yes |
No |
|
|
|
|
|
||
Do you serve children under age 18 who have special care needs because of a mental, physical, or emotional disability, requires specialized facilities, lower staff ratio, or specially trained staff to meet his/her developmental and physical needs?
Yes |
No |
|
|
|
|
|
|
|
|
|
|
|
|
If yes, is the rate for this child higher, lower, or the same for other children for whom you provide care? |
|
|
|||||||||||
Higher |
Lower |
Same |
|
|
|
|
|
|
|
||||
Do you participate in the Child and Adult Care Food Program? |
Yes |
No |
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Rates Charged Per Child |
|
|
|
|
|
|
|
|
|
|
|
||
You must complete both sections below, even if you do not currently care for a child in each age group. |
|
|
|||||||||||
Under 3 Years of Age: |
|
|
|
|
|
3 Years of Age and Over: |
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
$ |
|
|
per Day |
|
$ |
|
per Day |
|
|||||
Complete |
|
|
|
|
|
|
|
||||||
$ |
|
|
per Hour |
|
$ |
|
per Hour |
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
RETURN TO: |
|
|
||
PROVIDER SIGNATURE AND TITLE |
|
|
DATE |
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
PROVIDER DIRECTORY |
|
|
||
|
|
|
|
|
|
|
|
|
P.O. Box 94065 |
|
|
||
|
|
|
|
|
|
|
|
|
Baton Rouge, LA 70804 |
|
|
||
PRINT NAME |
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
||
CAPS/TIPS REPRESENTATIVE |
|
|
|
DATE |
|
|
|
|
|
|
|
||
|
|
|
|
1 |
|
|
|
|
|
|
|
||